

Acute pancreatitis (AP) in children in Japan is often caused by an anatomical abnormality of the pancreatic and bile duct, resulting in fever, abdominal pain, vomiting, diarrhea, and other symptoms1). Crohn’s disease (CD), however, is a chronic granulomatous inflammatory bowel disease (IBD) with ulcerative lesions of the intestinal tract of unknown cause that occurs mainly in young people, with symptoms similar to those of AP2). As most instances of CD gradually progress with the advancement of clinical symptoms, diagnosing CD in the preclinical stage can be challenging. Recently, fecal calprotectin was shown to be a noninvasive and useful biomarker in the diagnosis of IBD3). We describe a case of presymptomatic or mild CD that was diagnosed by measurement of fecal calprotectin level soon after the development of AP in a patient with incomplete pancreas divisum.
The content of research paper
Usefulness of Fecal Calprotectin Measurement in a Pediatric Patient with Crohn’s Disease
Shota Inoue, Kana Ito, Kiyotaka Zaha, Yusuke Yoshida, Yujin Sekinaka, Yoichi Kawamura
-
Shota Inoue
Department of Pediatrics, Japan Self Defense Forces Central Hospital
-
Kana Ito
Department of Pediatrics, Japan Self Defense Forces Central Hospital
-
Kiyotaka Zaha
Department of Pediatrics, Japan Self Defense Forces Central Hospital
-
Yusuke Yoshida
Department of Pediatrics, Japan Self Defense Forces Central Hospital
-
Yujin Sekinaka
Department of Pediatrics, Japan Self Defense Forces Central Hospital
-
Yoichi Kawamura
Department of Pediatrics, Japan Self Defense Forces Central Hospital
Introduction
Case report
A 14-year-old girl had been well until two weeks earlier when she began to experience diarrhea, fever, and abdominal pain. The fever subsided over one day, but the diarrhea and abdominal pain continued.
Her past medical history and family history were not significant. Diarrhea occurred 3-4 times a day, with watery stools and no gross hematochezia. Her height was 154.8 cm (−0.39 SD), weight was 42.5 kg (−1.15 SD), and her vital signs were stable. Physical examination revealed tenderness in the right lower abdomen and decreased intestinal peristalsis. There were no other findings of anorectal lesions or arthralgia. Laboratory results showed a lipase level of 811 U/L, amylase level of 309 U/L, and C-reactive protein (CRP) level of 1.08 mg/dL (Table 1). Contrast-enhanced computed tomography (CT) scan showed a pancreas of age-appropriate size, inflammation not extending beyond the pancreas, and no contrast-enhanced area, but edematous changes were observed in the perirectal wall (Fig. 1a, b). Abdominal echography showed an enlarged pancreatic head measuring 29.8 mm (Fig. 1c). Our patient presented with acute abdominal pain and elevated levels of pancreatic enzymes in the blood. In accordance with Japanese guidelines for the management of AP, a diagnosis of AP was established, with the severity determined to be mild at hospital admission. Thereafter, abdominal pain and diarrhea became mild by treatment only with bowel rest achieved by nothing per os (NPO), and her pancreatic enzymes tended to improve. A fat-controlled diet was started on day five of hospitalization, after which the amount of fat was gradually increased. Magnetic resonance cholangiopancreatography (MRCP) showed unclear delineation of a suspected incomplete pancreas divisum. Her clinical symptoms subsided, and she was discharged on hospital day eight on a continued fat-controlled diet. Immediately after discharge, however, the patient experienced recurrent epigastric and back pain after each meal, and diarrhea occurred 2-3 times per day. On day three after discharge, vomiting, epigastric pain, and back pain worsened, and the patient returned to the hospital the next day. Laboratory results showed lipase at 1649 U/L, amylase at 521 U/L, CRP at 2.46 mg/dL, and fecal calprotectin >6,000 mg/kg (Table 1). The patient was diagnosed as having a relapse of AP and was readmitted to hospital. As before, clinical symptoms subsided after she was placed on NPO status. After the symptoms became mild, abdominal echography showed no enlargement of the pancreatic head, and re-evaluation with MRCP showed delineation of the dorsal pancreatic duct and a meandering ventral pancreatic duct, which led to the diagnosis of incomplete pancreas divisum (Fig. 1d, e). Thereafter, the patient was started on a fat-controlled elemental diet, camostat mesilate, and Sanactase. Although there was no relapse of symptoms after increasing the fat dose, the pancreatic enzymes showed no tendency to decrease.
The patient’s high fecal calprotectin level and edematous wall thickening on CT raised the possibility that the IBD itself might have either coexisted with or caused the AP. Colonoscopy showed an ulcer on the lower lip of the ileocecal valve and deformity due to scarring of a recurrent ulceration along with circular shallow ulcers in the descending colon, sigmoid colon, and rectum (Fig. 2a-c). Upper gastrointestinal endoscopy revealed a bamboo sign from the curvature of the stomach to the cardia (Fig. 2d), but there was no gross lesion in the duodenum. Histological examination revealed noncaseating granulomas in the colon, stomach, and duodenum (Fig. 2e, f). Magnetic resonance enterography showed no abnormal dilation or stricture within the small intestine on hospital day 30. Thus, the patient met Japanese diagnostic criteria for CD and was diagnosed as having CD of mild-to-moderate activity. Prednisolone was administered with an induction dose of 20 mg. Her pancreatic enzymes improved, and she was discharged on hospital day 43. The prednisolone was tapered, a 5-ASA drug was introduced without symptom relapse, and her symptoms remained controlled. At 3 months from discharge, her abnormal pancreatic enzyme levels showed improvement (Table 1).
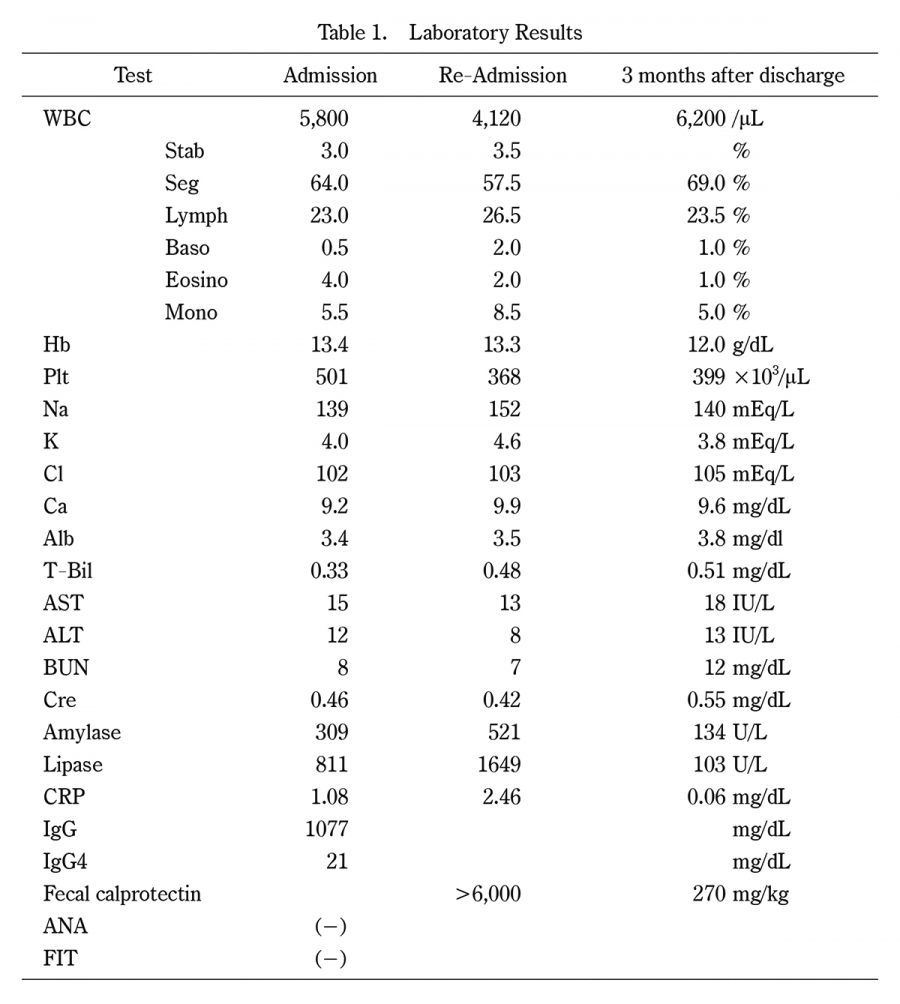
Table 1.
Laboratory Results
WBC:white blood cell, Hb:hemoglobin, Plt:platelet, Alb:albumin, T-Bil:total bilirubin, AST:aspartate aminotransferase, ALT:alanine, BUN:blood urea nitrogen, Cre:creatinine, CRP:C-reactive protein transaminase, IgG:immunoglobulin G, ANA:antinuclear antibody, FIT:fecal immunochemical test.
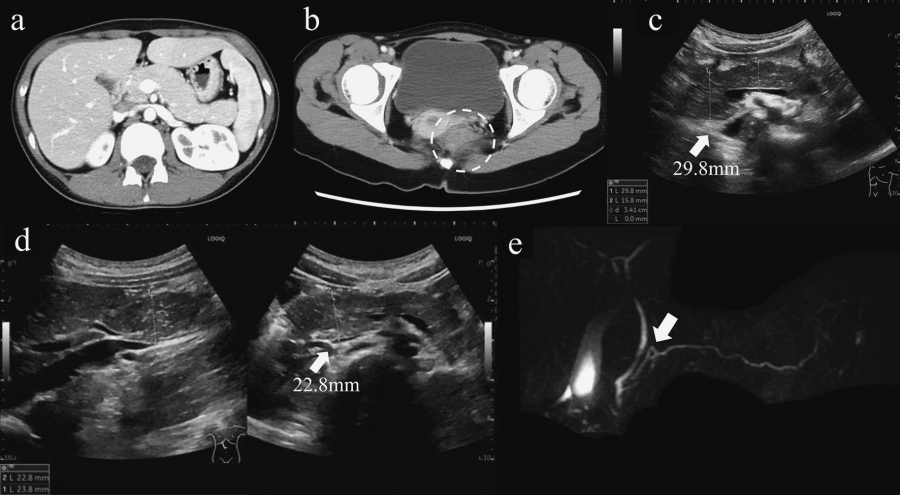
Fig. 1.
Computed tomographic (CT), abdominal echographic, and magnetic resonance (MR) cholangiopancreatographic findings.
(a) Contrast-enhanced CT scan of the abdomen on first admission. The pancreas was of an age-appropriate size and showed no contrast-enhanced area. Inflammation did not extend beyond the pancreas. (b) Contrast-enhanced CT of the abdomen on first admission. Edematous changes in the perirectal wall were observed (white dashed circle). (c) Abdominal echography on first admission. The pancreatic head was enlarged to 29.8 mm (white arrow). (d) Abdominal echography after relief of symptoms. The pancreatic head had shrunk to 22.8 mm, clearly smaller than in (c) (white arrow). (e) Magnetic resonance cholangiopancreatography showed that the dorsal pancreatic duct joins the main ventral pancreatic duct (white arrow).
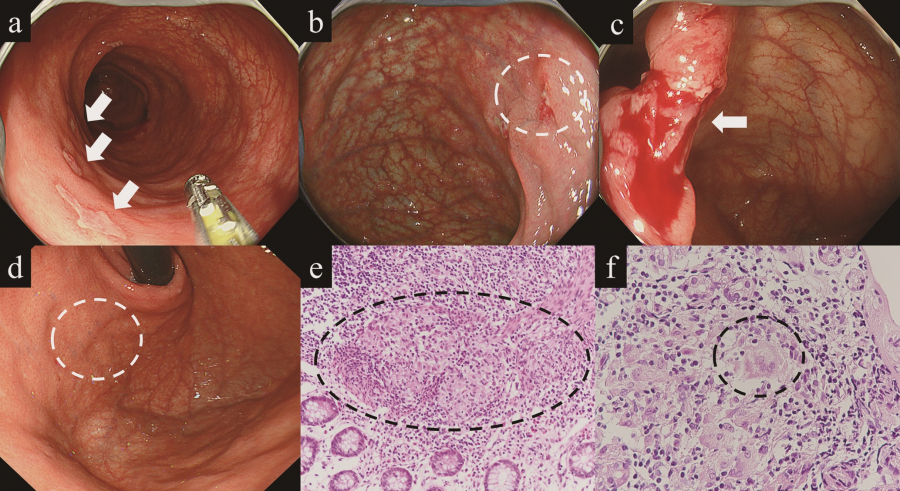
Fig. 2.
Colonoscopy and pathological findings.
(a) Colonoscopy. Circular shallow ulcers are scattered over the sigmoid colon (white arrows). (b) Colonoscopy. Circular shallow ulceration of the descending colon (white dashed circle). (c) Colonoscopy. Ulceration and deformity due to scarring suspected to be from recurrent ulceration of the inferior lip of the ileocecal valve (white arrow). (d) Upper gastrointestinal endoscopy. A bamboo sign is present from the curvature of the stomach to the cardia (white dashed circle). (e) Pathological findings from the colon (H & E stain, ×200). The histopathological image depicts noncaseating granulomas (black dashed circle). (f) Pathological findings from the stomach (H & E stain, ×400). The histopathological image similarly depicts noncaseating granulomas (black dashed circle).
Discussion
We encountered a case of pediatric AP with incomplete pancreas divisum and presymptomatic or mild CD. Although the diagnosis of presymptomatic or mild CD is challenging, as pediatricians, we should consider the coexistence of IBD in pediatric AP. Fecal calprotectin measurement offers the potential to diagnose and evaluate complications of IBD.
Pediatric AP results from multiple factors such as genetic causes, pancreatic anomalies, gallstones and microlithiasis, medications, and additional risk factors of trauma, metabolic disorders, infections, systemic disease, and autoimmune pancreatitis4). Our patient’s pancreatic anomaly had the potential to cause development of AP. A large study found a 1.5-to 4-fold increased risk of AP in patients with IBD compared with healthy controls, although the pathophysiology for this remains unknown5-8). In the present case, the exact relationship between her AP and CD remained unclear.
Calprotectin is a calcium-binding protein component of neutrophils and is released in the presence of inflammation. Calprotectin in stool correlates with neutrophil infiltration in the intestinal tract9). Fecal calprotectin is a useful tool with which to diagnose IBD along with endoscopic evaluation of disease activity in IBD3,10). In general, the gold standard for the diagnosis and evaluation of CD is endoscopy and histopathology, but these are invasive, expensive tests, and general anesthesia is sometimes required in children, making such tests not easily performed3). As most instances of CD gradually progress with the appearance of clinical symptoms, diagnosing CD in the preclinical stage can be challenging. In fact, it was difficult to determine the indication for endoscopy in our patient because her symptoms could be explained as the course of AP due to incomplete pancreas divisum. The diagnostic utility of fecal calprotectin showed excellent negative predictive value in ruling out IBD in symptomatic undiagnosed patients11). While only scattered data are present on optimal calprotectin threshold values in pediatric patients, the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition has reported a level of >250 mg/kg as being predictive of mucosal inflammation12). High fecal calprotectin levels and abnormal CT findings of edematous changes in the perirectal wall suggest the possibility of coexisting IBD. Because of the difficulty in diagnosing CD in the asymptomatic or early clinical stage, fecal calprotectin measurement in the screening of patients suspected of having IBD offers the potential to establish the coexistence of IBD accurately and quickly.
Informed consent
Written informed consent was obtained from the patient’s parents for publication of this case report.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgement
The authors thank Rise Japan LLC for carefully proofreading the manuscript.
Author contributions
S.I. wrote the manuscript. K.I., K.Z., Y.Y., Y.S., and Y.K. supervised the manuscript. All authors read and approved the final manuscript.