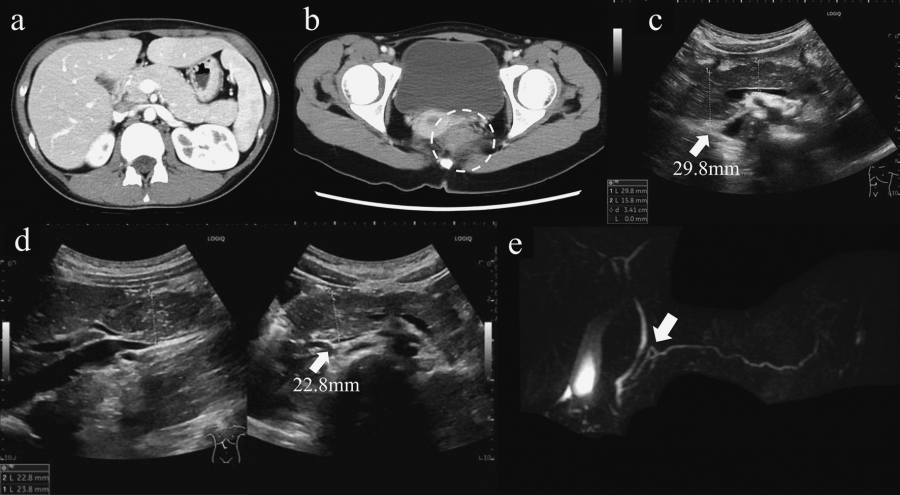
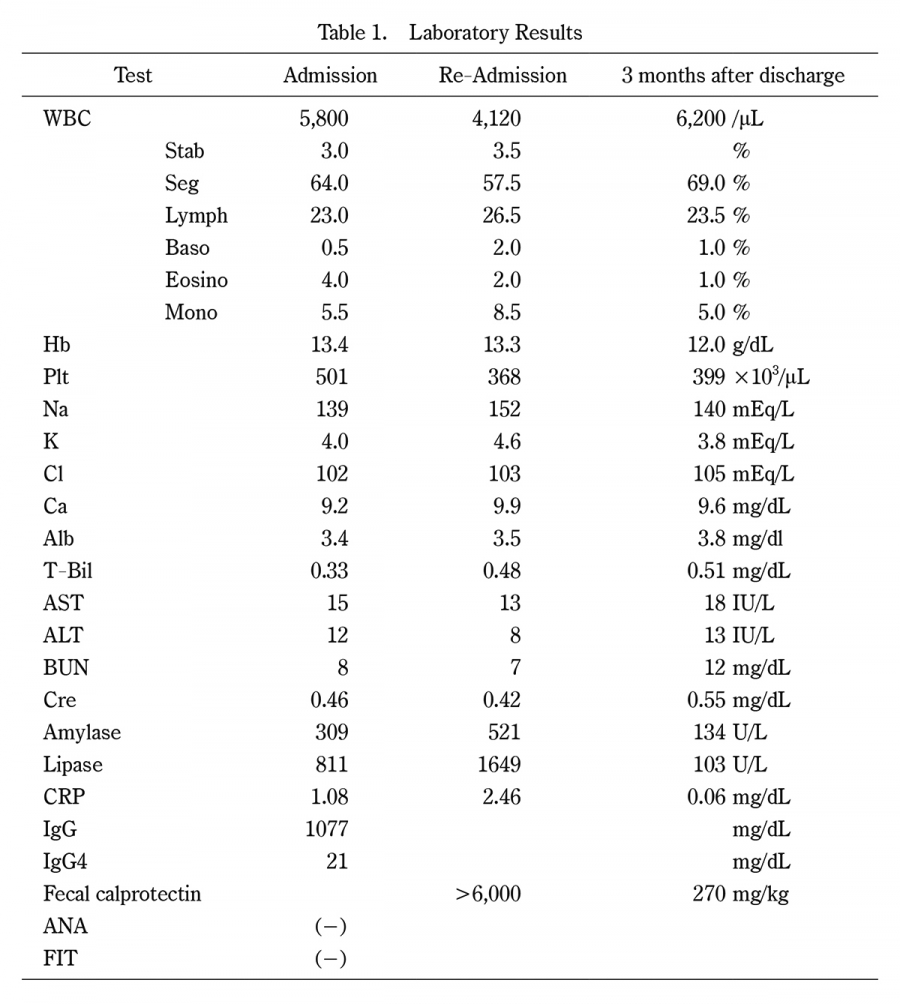
Acute pancreatitis in children in Japan is often caused by an anatomical abnormality of the pancreatic and bile duct, resulting in fever, abdominal pain, vomiting, diarrhea, and other symptoms. Crohn’s disease, however, is a chronic granulomatous inflammatory bowel disease with ulcerative lesions of the intestinal tract of unknown cause that occurs mainly in young people, with symptoms similar to those of acute pancreatitis. We report a case of acute pancreatitis diagnosed in a patient not only with incomplete fusion of the pancreatic duct but also with Crohn’s disease. A 14-year-old girl, healthy by nature, presented to our hospital with complaints of abdominal pain and diarrhea. She was initially diagnosed as having acute pancreatitis due to incomplete pancreas divisum. However, a high level of fecal calprotectin led to endoscopic examination, which resulted in the diagnosis of Crohn’s disease. Fecal calprotectin can be useful in the diagnosis of inflammatory bowel disease associated with acute pancreatitis in children. Although the relationship between inflammatory bowel disease and acute pancreatitis has not yet been clarified, we suggest that in the present case, acute pancreatitis may have manifested as a complication of Crohn’s disease and an underlying case of incomplete pancreas divisum.
Abstract/References
Usefulness of Fecal Calprotectin Measurement in a Pediatric Patient with Crohn’s Disease
Shota Inoue, Kana Ito, Kiyotaka Zaha, Yusuke Yoshida, Yujin Sekinaka, Yoichi Kawamura
-
Shota Inoue
Department of Pediatrics, Japan Self Defense Forces Central Hospital
-
Kana Ito
Department of Pediatrics, Japan Self Defense Forces Central Hospital
-
Kiyotaka Zaha
Department of Pediatrics, Japan Self Defense Forces Central Hospital
-
Yusuke Yoshida
Department of Pediatrics, Japan Self Defense Forces Central Hospital
-
Yujin Sekinaka
Department of Pediatrics, Japan Self Defense Forces Central Hospital
-
Yoichi Kawamura
Department of Pediatrics, Japan Self Defense Forces Central Hospital
Abstract
References
2. Kaser A, Zeissig S, Blumberg RS. Inflammatory bowel disease. Annu Rev Immunol, 28:573-621, 2010.
3. Fagerberg UL, Lööf L, Lindholm J, Hansson LO, Finkel Y. Fecal calprotectin:a quantitative marker of colonic inflammation in children with inflammatory bowel disease. J Pediatr Gastroenterol Nutr, 45(4):414-420, 2007.
4. Uc A, Husain SZ. Pancreatitis in Children. Gastroenterology, 156(7):1969-1978, 2019.
7. Munk EM, Pedersen L, Floyd A, Nørgård B, Rasmussen HH, Sørensen HT. Inflammatory bowel diseases, 5-aminosalicylic acid and sulfasalazine treatment and risk of acute pancreatitis:a population-based case-control study. Am J Gastroenterol, 99(5):884-888, 2004.
9. Røseth AG, Schmidt PN, Fagerhol MK. Correlation between faecal excretion of indium-111-labelled granulocytes and calprotectin, a granulocyte marker protein, in patients with inflammatory bowel disease. Scand J Gastroenterol, 34(1):50-54, 1999.
10. Dolwani S, Metzner M, Wassell JJ, Yong A, Hawthorne AB. Diagnostic accuracy of faecal calprotectin estimation in prediction of abnormal small bowel radiology. Aliment Pharmacol Ther, 20(6):615-621, 2004.
11. Konikoff MR, Denson LA. Role of fecal calprotectin as a biomarker of intestinal inflammation in inflammatory bowel disease. Inflamm Bowel Dis, 12(6):524-534, 2006.
Figures