In inflammatory bowel disease (IBD), including ulcerative colitis (UC) and Crohn’s disease (CD), a chronic inflammatory disorder of the intestinal mucosa causes repeated relapses and remissions, leading to the gradual accumulation of intestinal damage1). Prompt induction of remission and its sustained maintenance are essential treatment strategies to eliminate intestinal damage2, 3). Recent advancements in IBD treatment have been significant, though thiopurines remain key drugs4, 5). Thiopurines were originally developed as therapeutic agents for childhood leukemia6), and their immunomodulatory effects on IBD were initially reported in the late 1960s 7). Currently, thiopurines are used to maintain long-term, steroid-free remission and to prevent secondary failure of anti-tumor necrosis factor αagents in IBD patients8, 9).
Several enzymes are involved in the metabolism of thiopurines, including azathioprine (AZA) and 6-mercaptopurine (6-MP), and these metabolic enzymes can be affected by various agents, as illustrated in Figure 1. It is well known that two key drugs used in the treatment of IBD patients affect thiopurine metabolism10, 11). The first one is allopurinol, a uric acid synthesis inhibitor, which is metabolized to oxypurinol. Allopurinol exerts its effect on thiopurine metabolism by inhibiting both xanthine oxidase (XO) and thiopurine S-methyltransferase (TPMT)12). Through these two different pathways, allopurinol strongly increases the levels of 6-TGN, which is significantly and independently associated with the therapeutic response in IBD13). The second drug is 5-aminosalicylic acid (5-ASA), which interacts with thiopurine metabolism by inhibiting TPMT14). However, the effect of 5-ASA on thiopurine metabolism varies depending on the specific formulation, and the administration of time-dependent 5-ASA alone can impact thiopurine metabolism15).
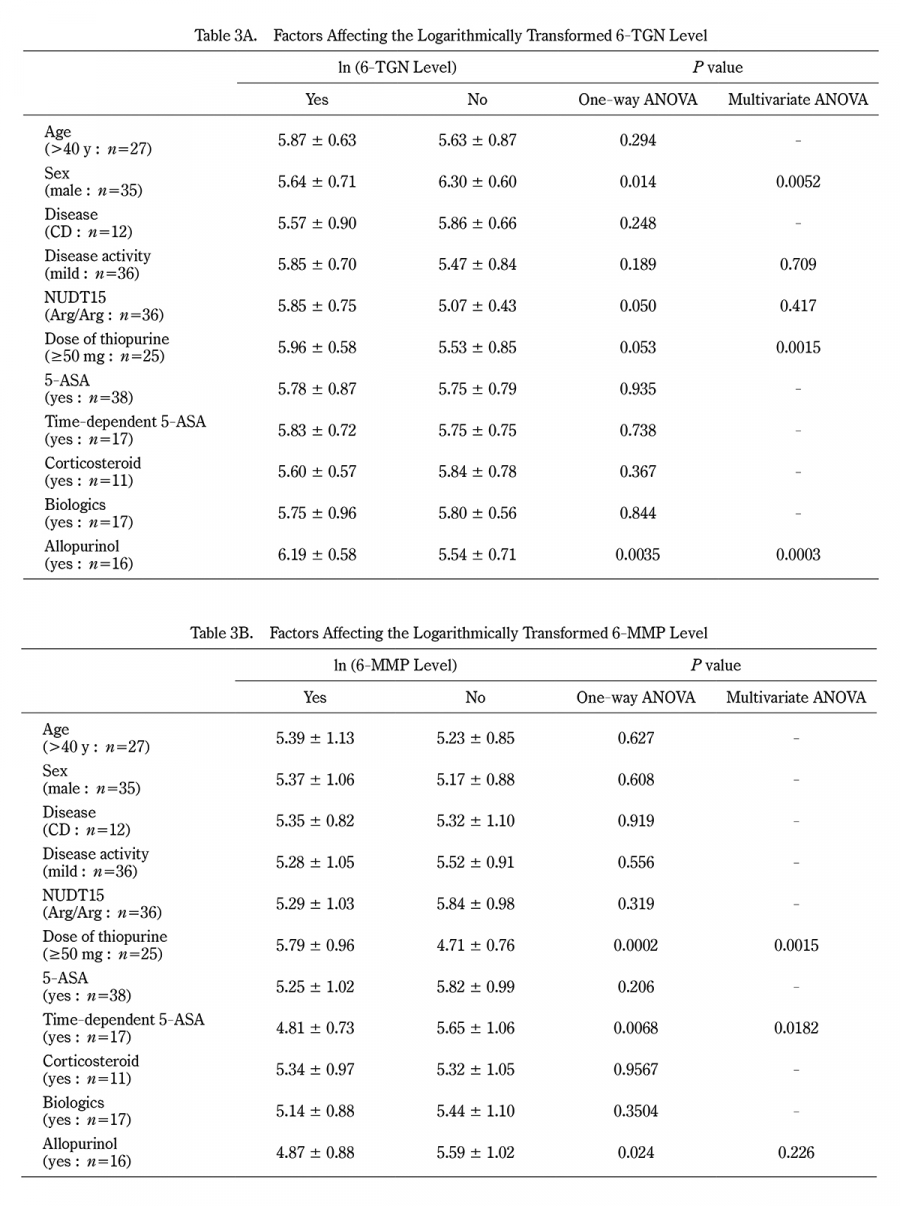
Apart from allopurinol and time-dependent 5-ASA, limited reports have examined the factors affecting the metabolism of thiopurines in real-world settings16,17). Furthermore, few reports have clarified the relationships between the concentrations of thiopurine metabolites and sex, age, NUDT15 (nucleoside diphosphate-linked moiety X-type motif 15), etc. This study focused on the intracellular concentrations of 6-TGN and 6-MMP associated with hepatoxicity and investigated the effects of concurrent medications and patient characteristics on the intracellular concentrations of 6-TGN and 6-MMP in IBD patients undergoing thiopurine therapy.
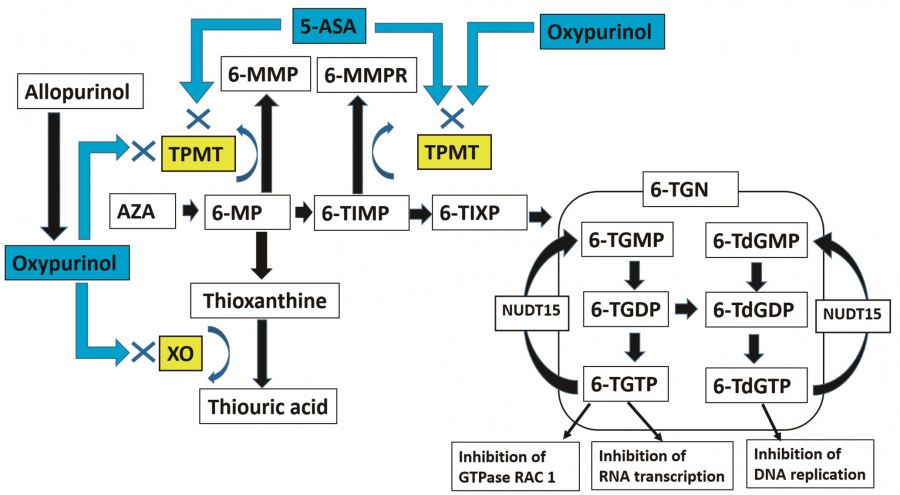
Fig. 1.
Thiopurine metabolism. Metabolic enzymes are marked in yellow, and drugs related to them are marked in blue. 5-ASAs are thought to contribute to the increase in 6-TGN concentration by reducing 6-MMP by inhibiting TPMT activity. 6-MP has another pathway to be metabolized to thiouric acid via thioxanthine. Oxypurinol, a metabolite of allopurinol, causes elevation of thioxanthine by inhibiting xanthine oxidase (XO), which metabolizes thioxanthine. Oxypurinol also has an inhibitory effect on TPMT. Through these two mechanisms, allopurinol exerts a strong 6-TGN-increasing effect. AZA is non-enzymatically degraded to 6-MP and finally metabolized to 6-thioguanine nucleotide (6-TGN) via 6-thioinosine monophosphate (6-TIMP). 6-TGN inhibits intracellular nucleic acid synthesis and protein synthesis, thus suppressing the proliferation of activated lymphocytes. Thiopurine methyltransferase (TPMT) is an enzyme converting 6-MP to 6-methylmercaptopurine (6-MMP) and 6-TIMP to 6-methylmercaptopurine ribonucleotide (6-MMPR), and both metabolites (6-MMP and 6-MMPR) are associated with hepatotoxicity.