The purpose of this study was to conduct a detailed retrospective review of preoperative MRI findings and postoperative pathology in 170 cases of uterine tumors, with the goal of determining how to avoid missing sarcoma cases when performing a differential diagnosis of uterine sarcoma and leiomyoma (especially, differentiation from cellular leiomyoma and degenerated leiomyoma). MRI is useful in the diagnosis of uterine tumors, especially in the differential diagnosis of leiomyoma and uterine sarcoma. Several recent reports have discussed distinguishing these tumors by using DWI and ADC to compare biofunction4).
Ando et al. reported that the presence of a T1WI high-intensity signal area (T1-HIA) within a uterine tumor was important in differentiating leiomyoma from LMS on MRI, and such areas were found in 1.3% of 490 leiomyoma cases compared to 78.6% of 14 LMS cases6). Furthermore, there were significant differences between leiomyoma and LMS in terms of the occupying rate of T1-HIA (0.20±0.24 vs 0.42±0.27, respectively, p<0.05), homogenous signal uniformity (53% vs 0%, respectively, p<0.01), and well-demarcated margins (60% vs 9%, respectively, p<0.05)6). Another study reported that T1-HIA in LMS reflects coagulative necrotic foci (tumor cell necrosis) within the tumor and is highly suggestive of malignancy, unlike infarct-type necrosis (hyaline necrosis) in leiomyoma, which reflects granulation and vitrification due to hemorrhage4,9).
Several papers have reported the usefulness of contrast-enhanced MRI (CE-MRI) in differentiating sarcomas (LMS/STUMP) from leiomyoma10,11). Lin et al. showed that CE-MRI findings, especially central nonenhancement (CNE) findings, were of greater diagnostic value than DWI, T1WI, and T2WI results for the differential diagnosis of 25 rapidly enlarging leiomyomas and 8 LMS/STUMP cases10). The authors also reported that the combination of DWI and ADCVs (with the cut-off value of the latter set at 1.08×10-3 mm2/s) provided diagnostic value equivalent to that of CE-MRI, which is useful for patients with suspected sarcoma but who have renal dysfunction that prevents the use of contrast agents.
Distinguishing between degenerated leiomyoma and sarcoma can sometimes be difficult, and DWI and ADCVs can be useful in this regard. Generally, increased cell number and volume, high nuclear-to-cytoplasmic ratio, and limited diffusion of water molecules due to a small extracellular lumen in uterine sarcoma are reflected as decreased ADCVs8). Regarding the usefulness of ADCVs, Li et al. analyzed 16 LMS and 26 DLM cases and found that the median ADCV was significantly lower in LMS than in degenerated leiomyoma (0.81±0.14 vs 1.22±0.22×10-3 mm2/s, respectively, p<0.001)8). Furthermore, in an analysis of 33 cases of rapidly enlarging uterine tumors, Lin et al. reported that the mean ADCV was significantly lower in 8 LMS/STUMP cases than in 25 degenerated leiomyoma cases (0.89 vs 1.19×10-3 mm2/s, respectively, p<0.05)10).
Wahab et al. developed an algorithm to differentiate between 51 cases of uterine sarcoma and 106 cases of benign atypical leiomyoma12). First, according to their algorithm, sarcoma is strongly suspected when lymph node enlargement or peritoneal dissemination is present. Second, the combination of T2WI, DWI, and ADCV (cut-off:0.905×10-3 mm2/s) is used to diagnose a tumor as highly suspect, certainly benign, or probably benign. The sensitivity and specificity of their algorithm for the diagnosis of malignancy were >83% and >94%, respectively, which indicates good accuracy. In short, they reported that in atypical uterine tumors, high T2WI signal intensity (T2WI-high), DWI-high, and an ADCV ≤0.905×10-3 mm2/s were highly suggestive of sarcoma12). There are several reports on the optimal ADCV cut-offs (1.06-1.23 mm2/s) for the differentiation of uterine sarcomas8,10,12). Wahab et al. pointed out that a higher ADCV cut-off increases the negative predictive value, but its drawback is that unnecessary total hysterectomy may be performed because a benign leiomyoma is deemed suspicious of malignancy12).
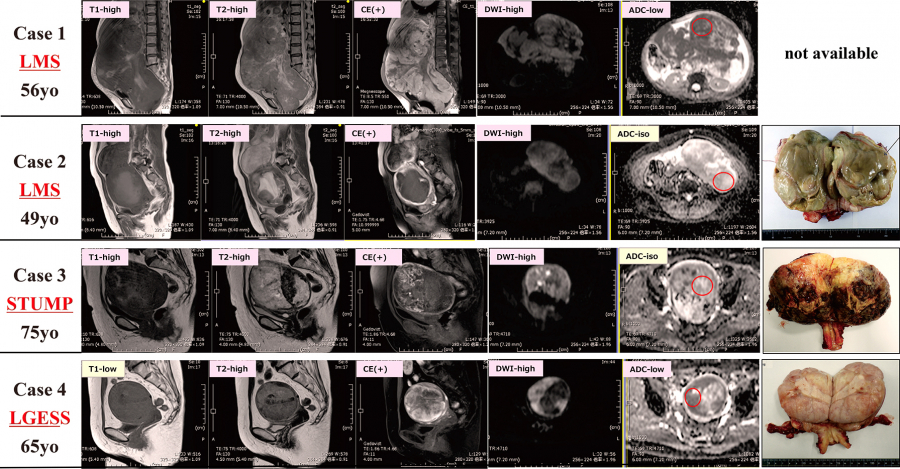
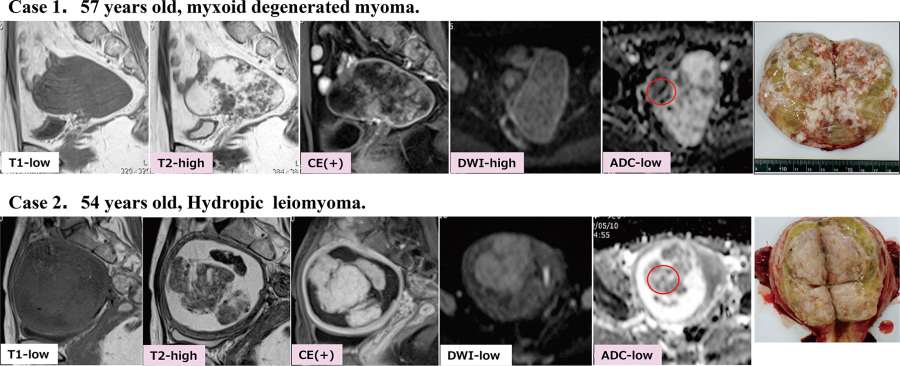
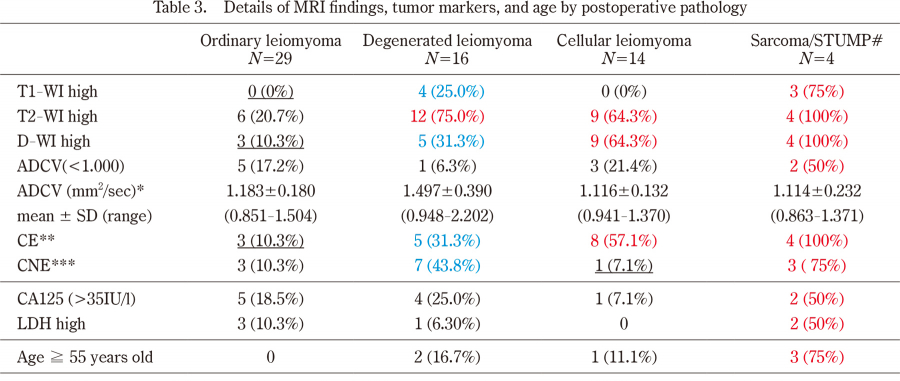
As mentioned above, MRI findings that are particularly useful in differentiating atypical leiomyoma from sarcoma include T1-HIA, CE on CE-MRI, CNE, and diffusion limited and reduced ADCV on DWI6,8,10,11). In this study, the 4 sarcoma/STUMP cases that are shown in Figure 1 also exhibited high rates of T1-HIA (75%), CE (100%), CNE (75%), DWI-high (100%), and low ADCV (50%), but not all findings were necessarily present, even in sarcoma cases (especially in LGESS, which had fewer findings). A well-known and characteristic finding on MRI images of LGESS is a “worm-like” multinodular mass extending into the myometrium, suggesting invasion into the tumor with an intervening normal muscle layer4). Although the diagnosis is simple when such typical findings are present, differentiation from leiomyoma or adenomyosis is often problematic because of the difficulty in capturing invasive growths and the fact that LGESS often occurs at a younger age4).
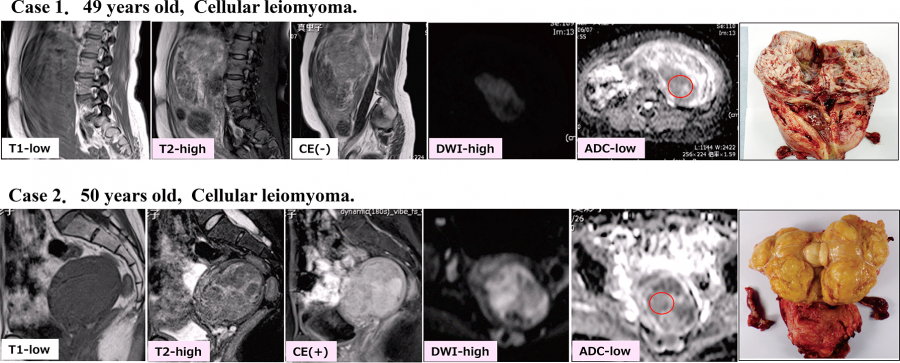
The results of this study showed that in ordinary leiomyoma, the incidence of abnormal findings was low;in degenerated leiomyoma, T2WI-high was highly prevalent (75%) while high T1 signal intensity (T1WI-high), DWI-high, CE-positive status, and CNE occurred in 25-44% of cases;and in cellular myoma, T2WI-high, DWI-high, and CE-positive status were highly prevalent (Table 3). As in previous reports8,10), the mean ADCV was significantly higher in degenerated leiomyoma than in other histological types (Figure 4), and ADCV was useful for differentiating degenerated leiomyoma from sarcoma, which are difficult to differentiate by other findings. Although the exact mechanisms remain unclear, it is possible that degenerated leiomyomas have abundant water content and are enriched in extracellular matrix with abundant collagen within the legions, and less limited diffusion of water molecules due to a larger extracellular lumen, which may result in increased ADCVs than in other histologic types8,13,14).
Based on the above MRI findings, the possibility of sarcoma was suspected in 16 (9.5%) of 169 cases operated on at our hospital, and intraoperative rapid pathology was performed;the details are shown in Table 4. All 3 sarcoma/STUMP cases were preoperatively suspected of being degenerated leiomyoma, but the possibility of sarcoma could not be ruled out. Intraoperative pathology examination was performed in 44% of cases of degenerated leiomyoma and 21% of cases of cellular myomas. Three cases of normal myoma were also diagnosed, all of which occurred in postmenopausal women (61, 62, and 69 years of age) with large tumors.
Other MRI findings that are usually useful in differentiating sarcoma from leiomyoma include tumor diameter, tumor margin (clear or indistinct), and tumor content (homogeneous or heterogeneous). In addition to imaging results, patient age, menopausal status, and the elevation of tumor markers such as CA125 or LDH have been reported as useful differentiating factors6,8);thus, also considering these may improve the accuracy of sarcoma diagnosis.
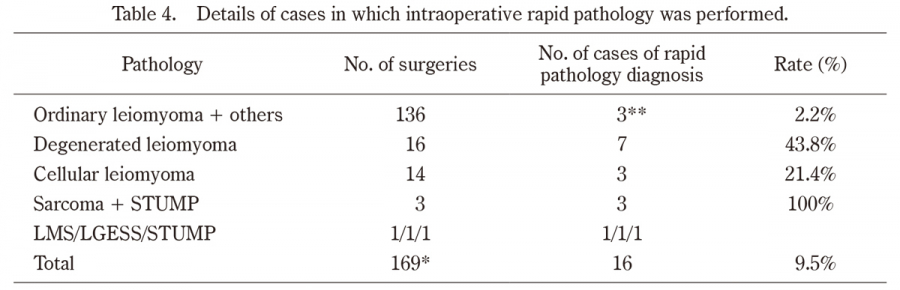
Table 4.
Details of cases in which intraoperative rapid pathology was performed.
*Total surgery cases in Fukushima Red Cross Hospital (169 cases).
**Ordinary leiomyoma cases were all in menopausal with large tumor (61, 62, and 69 years old, respectively).