The study was performed to investigate and compare attitudes toward schizophrenia among medical students, psychiatrists, psychiatric staff (other than psychiatrists), physicians, and non-medical workers.
Study Design
A web-based survey tool was used to create and conduct a survey of the study participants at Fukushima Medical University in Fukushima, Japan. Study participants were 490 medical students in their third to sixth year of medical training, 13 psychiatrists, 25 psychiatric staff members, 48 physicians, and 222 non-medical workers, such as office workers at the General Affairs Division of the university. Of the 490 medical students, 133 were third-year, 147 were fourth-year, 100 were fifth-year, and 110 were sixth-year students.
In Japan, medicine is a 6-year academic degree program that includes a 2-year pre-clinical stage followed by a 4-year clinical stage. Psychiatric classes that cover schizophrenia are given during the fourth year and consist of classroom lectures on the pathology, symptoms, and treatment of schizophrenia. Psychiatric practical training is provided in the fifth year and consists of clinical lessons (bedside learning [BSL]) on the clinical characteristics of mental disorders and their biopsychosocial treatments. Since psychiatric practical training also includes clinical workshops and attendance at clinical facilities at the Department of Psychiatry at the University Hospital, medical students have the opportunity to speak directly with and spend time with patients with schizophrenia during BSL. Therefore, all fifth-year students who participated in this survey had previously completed classroom psychiatry lectures, and all sixth-year students had previously received psychiatric practical training.
All study participants were Japanese, belonged to one of the 5 participant groups, and had agreed to complete web-based surveys provided as questionnaires on Google Forms (an online questionnaire format service provided by Google). All participants received a hyperlink to Google Forms via email containing various questionnaires. No identifying information (e.g., name or date of birth) was required of study participants. The study was conducted from September to December 2016. The study received ethics approval from the Fukushima Medical University Ethics Committee (approval #2736).
Survey and Questionnaires
The survey used in this web-based study comprised three sections:demographic information, knowledge about schizophrenia, and attitudes toward schizophrenia, which were measured using 18 items.
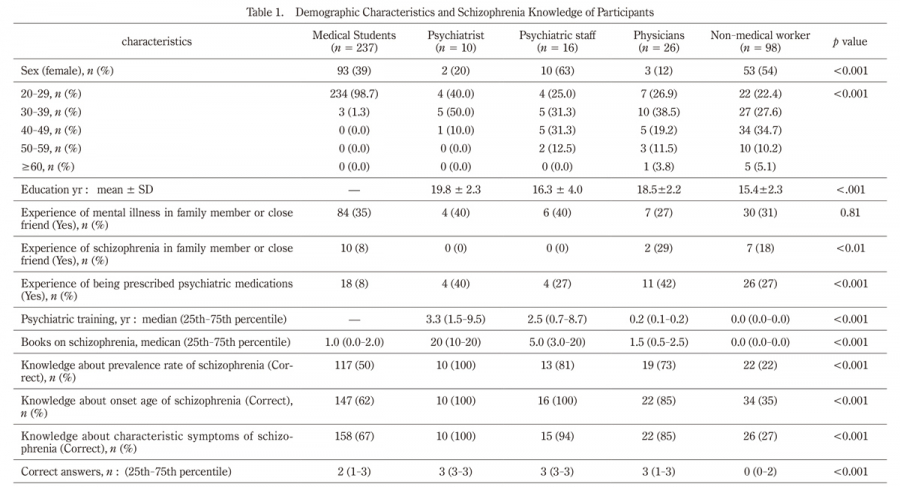
The demographic information collected from potential study participants included age, sex, number of years of education, number of years of psychiatric education, number of books read on schizophrenia, and occupation/qualifications (medical students, psychiatrists, psychiatric staff other than psychiatrists, physicians other than psychiatrists, and non-medical workers). The demographic questionnaire also asked if any family member or close friends had experienced psychiatric illness (“Do you have family or close friends with a history of psychiatric illness?”);if any family members or close friends had been diagnosed with schizophrenia (“Does that include individuals with schizophrenia?”);and whether participants had been prescribed psychiatric medications (“Have you ever been prescribed psychiatric medications, such as anxiolytics, hypnotics antidepressants, antipsychotics, and/or anticonvulsants?”). Finally, for potential medical student participants, the following additional information was collected:year of medical training at Fukushima Medical University;experience of taking psychiatric classes about schizophrenia at Fukushima Medical University (“Have you ever completed a psychiatry class on schizophrenia?”);BSL experience during the psychiatry term at Fukushima Medical University (“Have you completed BSL training during your psychiatric term?”);and hopes of becoming a psychiatrist (“Do you want to become a psychiatrist in the future?”).
Participants’ knowledge of schizophrenia was evaluated by three questions, each of which had 5 response options (1 correct answer and 4 incorrect answers). The first question was “Please select the approximate prevalence rate of schizophrenia”; the response choices were:1/50, 1/100 (correct answer), 1/300, 1/1,000, or “I don’t know.” The second question was “What is the typical age of schizophrenia onset?”;the response choices were: childhood, adolescence to early adulthood (correct answer), late adulthood, middle age, or “I don’t know.” The third question was “What is the characteristic symptom of schizophrenia?”;the response choices were panic attack, visual hallucinations, auditory hallucinations (correct answer), obsessive-compulsive behavior, or “I don’t know.” Participants were instructed to answer these questions without referring to any materials, including books.
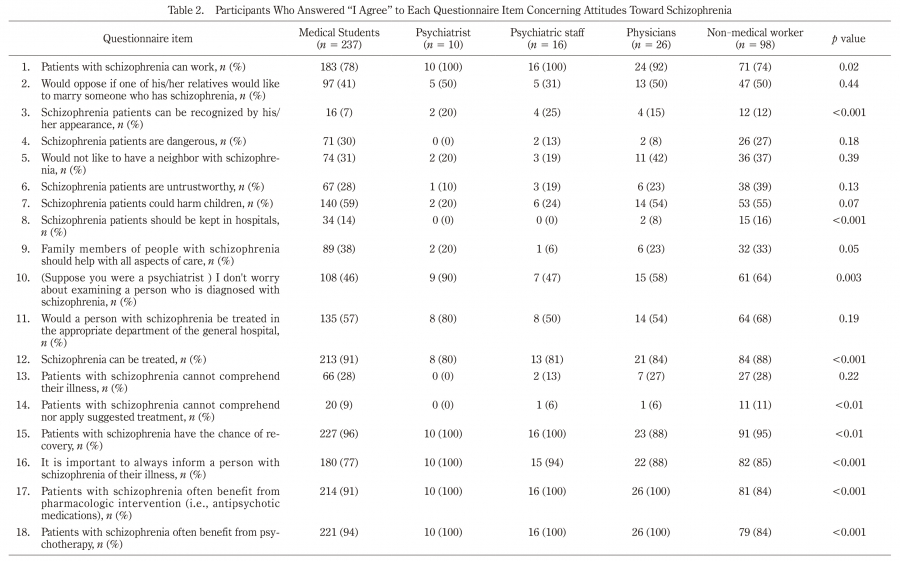
To evaluate attitudes toward schizophrenia, an 18-item questionnaire was created initially based on a study approach by Hori et al.9). That study questionnaire was based on the 13-item questionnaire developed by Uçok et al.7). The reliability and validity of the Japanese version have been reported elsewhere9). For the present study, an additional 5 items were added by referring to several other previous studies on attitudes toward schizophrenia17-20), resulting in the current 18-item questionnaire, presented in Table 2.
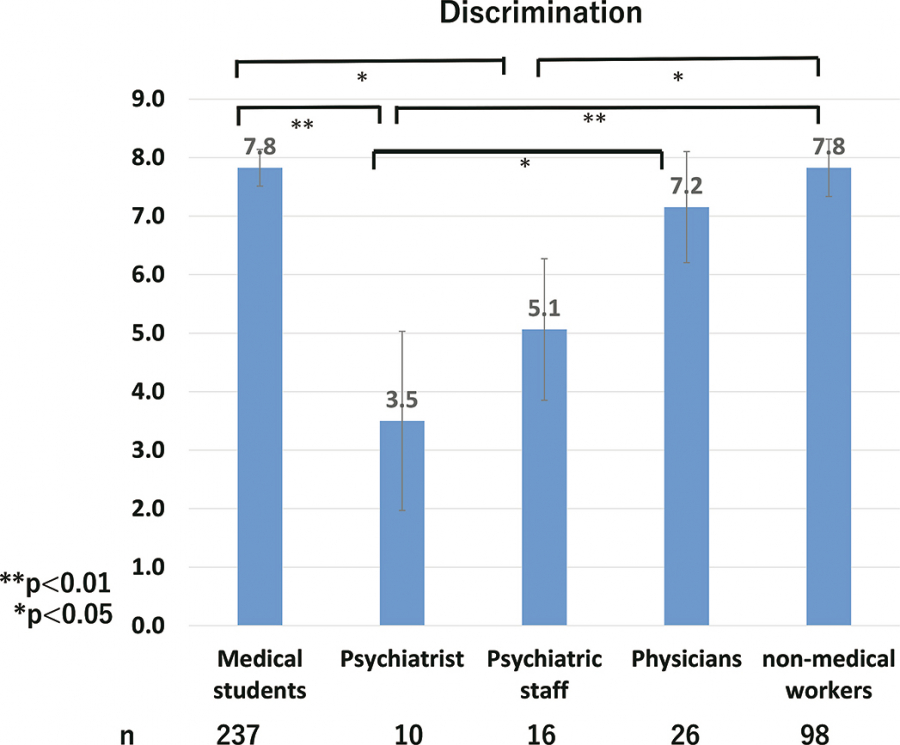
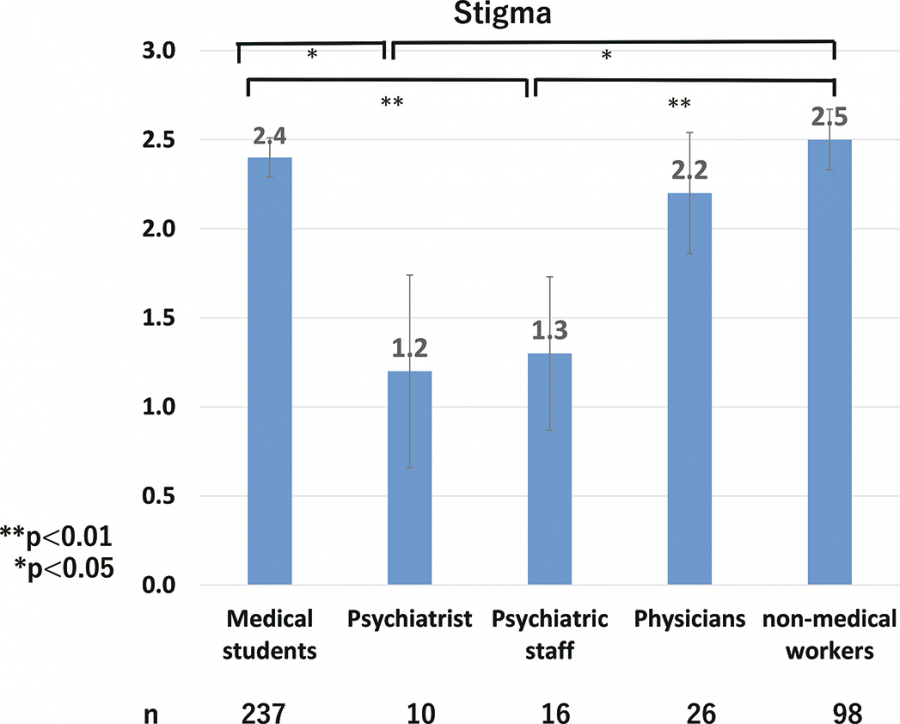
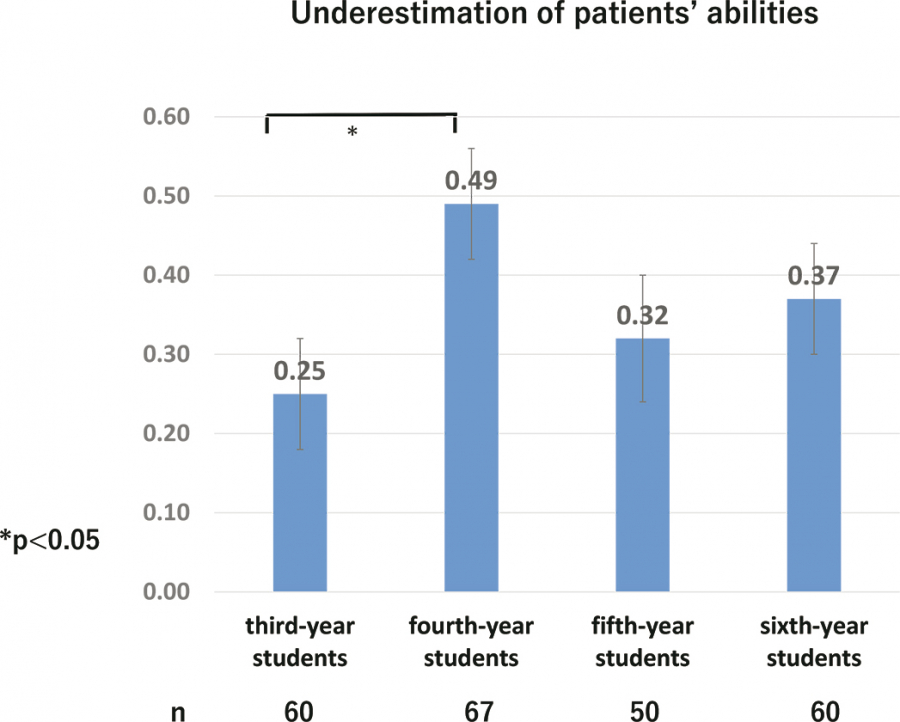
Participants were asked to answer each question with either “I agree” or “I disagree.” For items 1, 10, 11, 12, 15, 16, 17, and 18, responses of “I agree” were scored 0 and items answered with “I disagree” were scored 1. For the other items (2, 3, 4, 5, 6, 7, 8, 9, 13, and 14), the scoring was reversed. Therefore, for all items a higher score indicated a more negative attitude. The total score for each item was defined as the discrimination score. The questionnaire focused on 3 factors:9)stigma, underestimation of patients’ abilities, and skepticism regarding treatment. The summed scores for each factor were defined as the stigma score, underestimation of patients’ abilities score, and skepticism regarding treatment score.
Statistical Analysis
For continuous variables, the means and standard deviations were calculated;for ordinal variables, the medians were calculated (25th-75th percentiles). For categorical variables, data were reported as percentages. Means, medians, and categorical variables were compared using the analysis of variance (ANOVA), the Kruskal–Wallis test, Fisher’s exact test, and the χ2test. The differences among the five groups were also compared using the analysis of covariance (ANCOVA) adjusted for age and sex. When significant differences were obtained among the five groups, post hoc multiple comparisons by the Tukey test were performed to determine where the differences occurred among the five groups. The same method was used to analyze comparisons between grades among medical students.
Statistical significance was determined by a two-tailed test, with p< 0.05 as statistically significant and p< 0.1 as borderline statistically significant. Analyses were performed using the SAS, version 9.4 (SAS, Cary, North Carolina, USA).