

Heart failure (HF) is a clinical syndrome presenting with symptoms and/or signs caused by structural and/or functional cardiac abnormalities, and is characterized by elevated blood levels of natriuretic peptide and/or objective evidence of cardiogenic pulmonary or systemic congestion1,2). Hemodynamic features of HF can be described by a two-by-two matrix based on the presence/absence of congestion (‘wet’ vs. ‘dry’) and peripheral hypoperfusion (‘cold’ vs. ‘warm’)3,4). Pathophysiologically, HF is characterized by activation of various neuro-hormonal systems such as the renin-angiotensin-aldosterone system, the sympathetic nervous system, and vasopressin,5) resulting in hemodynamic changes that can seriously affect other organs such as the lungs,6,7) liver,6,8) kidneys,6,9) and intestines6,10). Our research group has conducted various clinical studies on HF, aiming to clarify the impact of HF on other organs and associated pathophysiology.
The content of research paper
Organ injury and its management in heart failure: Liver, kidney, and thyroid gland dysfunction
Yu Sato, Akiomi Yoshihisa, Yasuchika Takeishi
-
Yu Sato
Department of Cardiovascular Medicine, Fukushima Medical University
-
Akiomi Yoshihisa
Department of Cardiovascular Medicine, Fukushima Medical University
Department of Clinical Laboratory Sciences, Fukushima Medical University
-
Yasuchika Takeishi
Department of Cardiovascular Medicine, Fukushima Medical University
Introduction
Relationships between HF and other organs
Possible impacts of hemodynamic changes associated with HF on other organs are illustrated in Figure 1. These next paragraphs describe the relationship of HF with the liver, kidney, and thyroid gland. HF causes liver dysfunction through reduced arterial perfusion and/or passive congestion11-13). A previous report showed that arterial hypoperfusion, which is particularly predominant in acute HF, can lead to hypoxic hepatitis, whereas passive congestion in chronic HF induces congestive hepatopathy11). These forward and backward failures often coexist14). The latter may lead to liver stiffness, further resulting in fibrosis and adverse prognosis11-13). One of our studies investigated hemodynamic changes in the liver in HF patients and subsequent pathophysiological changes using non-invasive approaches. Based on previous studies reporting that elevated central venous pressure increases liver stiffness,15,16) we extrapolated the Fibrosis-4 (FIB4) index – computed from age and blood tests to assess the fibrosis or stiffness in patients with non-alcoholic fatty liver disease – to patients with HF17). HF patients in the highest tertile of the FIB4 index exhibited the highest liver fibrosis markers in blood, and echocardiography also revealed the most severe volume overload of the right heart17). The FIB4 index also showed that all-cause mortality significantly increased with increasing FIB4 scores17). Another approach we used to evaluate hemodynamics of liver in HF patients was abdominal ultrasonography18). Analysis of findings from cardiac catheterization and abdominal ultrasound showed that peak systolic velocity of the celiac artery and liver shear wave elastography had strong correlation with liver hypoperfusion and congestion, respectively18). From these results, we proposed a new hemodynamic classification of HF similar to the Nohria-Stevenson classification,19-23) which is non-invasive and has higher generalizability because it is based on ultrasonography, an objective and easy-to-perform technique. Compared to invasive cardiac catheterization, this new method improves the safety of patient management and allows easy and non-invasive reassessment whenever patient’s condition changes.
As for the relationship between HF and the kidneys, cardiac and renal diseases frequently coexist in what is known as cardio-renal syndrome (CRS)9,24). CRS is subdivided into five subtypes according to the speed and order of onset of the disorders9,24). For example, CRS type 1 is characterized by worsening renal function (WRF) due to acute HF, while in CRS type 2 chronic cardiac function abnormalities cause progressive chronic kidney disease9,24). Our analysis of data from the JASPER registry,25) a Japanese nationwide database of HF patients with preserved ejection fraction (HFpEF), revealed that HFpEF patients who experienced WRF during hospitalization had higher systolic blood pressure upon admission26). Additionally, these patients exhibited a higher prevalence of atherosclerotic comorbidities and more frequent signs of hypoperfusion throughout their hospital stay26). The analysis also suggests that diuresis and impaired fluid refilling from the extravascular space to the intravascular area can cause CRS type 1 in patients with HFpEF and history of atherosclerotic disease26). Thus, we emphasize the importance of careful monitoring to avoid excessive blood pressure decrease and over-diuresis in patients with HFpEF in terms of WRS from the study. Again, we used abdominal ultrasonography to visually assess the renal hemodynamic changes in HF patients in a non-invasive manner27). We found that renal artery flow and the intrarenal venous flow pattern correlate with cardiac index values and right atrial pressure, respectively27). It was also revealed that the renal venous stasis index reflects right-sided overload and is associated with adverse prognosis28).
The thyroid gland and the heart also have pathophysiological connections. For example, thyroid hormones have genomic and nongenomic effects on the heart and cardiovascular system. Triiodothyronine (T3) increases heart rate, left ventricular contractility, and blood volume while it decreases systemic vascular resistance and right atrial pressure29). Thyroid functions can be classified based on serum levels of thyroid stimulating hormone and free thyroxine29). Among HF patients (Figure 2), thyroid function testing found that the majority (82.8%) were euthyroid, and the most prevalent thyroid dysfunction was subclinical hypothyroidism (12.0%),30) slightly higher than the generally reported prevalence of 5-10%31). HF patients with subclinical hypothyroidism showed lower exercise capacity, higher pulmonary arterial pressure, higher incidence of cardiac events, and higher mortality compared to euthyroid patients, while left ventricular contractility was comparable30). In addition, T3 levels decrease due to the reduction of 5’ monodeiodinase in euthyroid patients with severe conditions that include HF32,33). This low T3 syndrome is known as “non-thyroidal illness syndrome” or “euthyroid sick syndrome”32). In our observational study, approximately one third of euthyroid patients hospitalized for HF showed low T3 syndrome (Figure 2)34). Patients with low T3 syndrome manifested more congestion and myocardial damage, as suggested by the levels of B-type natriuretic peptide (BNP) and troponin I, respectively34). These patients also showed lower nutritional status, impaired exercise capacity, and higher incidence of cardiac and all-cause deaths34). These results emphasize the importance of the assessment of thyroid disorders in patients with HF, and were cited in the European Society of Cardiology guidelines for HF4,35).
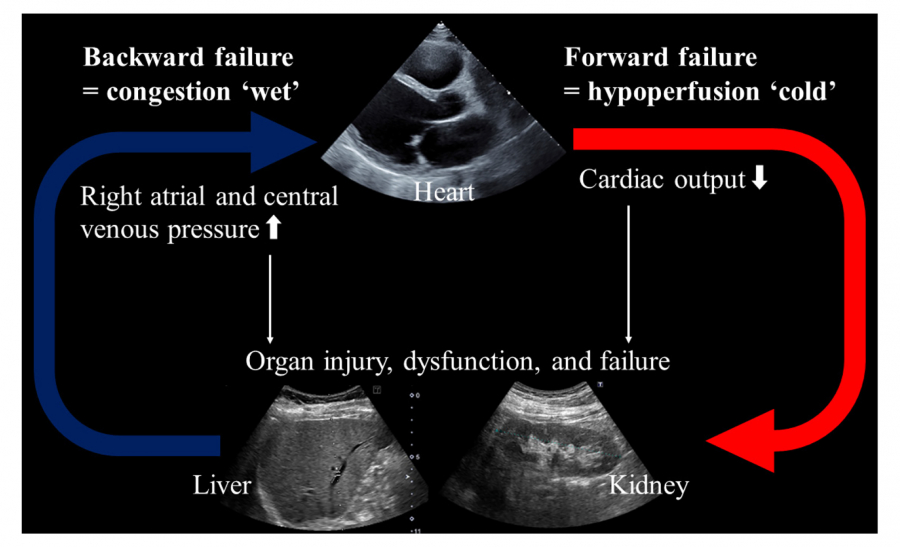
Fig. 1.
Hemodynamic features of HF
HF, heart failure.
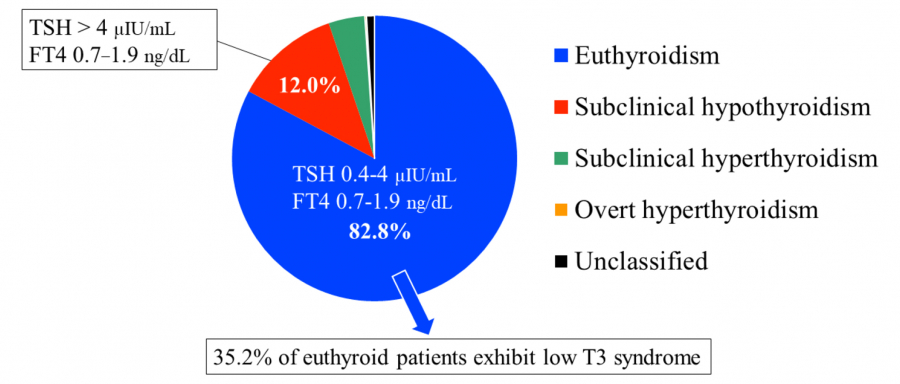
Fig. 2.
Thyroid function in patients with HF
HF, heart failure; TSH, thyroid stimulating hormone; FT4, free thyroxine, T3; triiodothyronine.
Adapted from Refs. 30 and 34.
Other considerations on pathophysiology associated with HF
Patients with HF sometimes suffer from non-cardiovascular comorbidities, some of which have similar pathophysiology, including neuro-hormonal activation4,36,37). For example, both HF and insomnia are associated with increased activity of the sympathetic nervous system, the hypothalamic pituitary adrenal axis, and the renin-angiotensin-aldosterone system38,39). Insomnia is prevalent in approximately 6-10% of the general population,40) and it not only deteriorates quality of life, but also increases risks of depression,41) HF,38) and mortality42). We conducted a questionnaire-based survey on insomnia among HF patients, and found two-thirds of them had insomnia43). Since benzodiazepines, the most widely prescribed class of hypnotics, have been attracting attention for their side effects,44) we evaluated the adverse effects of benzodiazepines in patients with HF. Compared to patients on non-benzodiazepines (zolpidem, zopiclone, or eszopiclone), those on benzodiazepines showed higher incidence of rehospitalization for HF after the propensity score matching for the choice of hypnotics43). After adjustment for confounding factors, the use of benzodiazepines resulted in 1.5-fold greater risk of rehospitalization for HF patients compared to the use of non-benzodiazepines43). These results suggest non-benzodiazepines should be preferred to benzodiazepines to avoid rehospitalization for HF. Moreover, there are some modifiable factors in addition to the selection of hypnotics. Since cognitive behavioral therapy is the first-line treatment for insomnia,45) collaboration with specialists such as psychiatrists should be considered. Medical therapy for HF can be optimized from the perspective of treating insomnia. For example, use of diuretics should be adjusted to avoid nocturnal dyspnea due to congestion and to avoid sleep disturbance due to nocturnal diuresis.
Cachexia, a complex metabolic syndrome characterized by loss of muscle with or without loss of fat mass, is caused by chronic illnesses including HF, cancer, and chronic kidney disease46,47). Cachexia associated with chronic HF is called cardiac cachexia, and occurs in 5-15% of patients with HF47). Patients with cardiac cachexia are likely to be at a more advanced stage4) and likely to have poor prognosis48,49). Since cardiac cachexia has multiple underlying pathophysiological factors, we evaluated the interactions between cardiac cachexia and coexisting prognostic risk factors. Among hospitalized patients with HF, 10.9% were diagnosed with cardiac cachexia, and the cardiac event and all-cause death rates were higher in patients with cardiac cachexia compared to those without cardiac cachexia50). Sex, cancer, use of loop diuretics, and levels of estimated glomerular filtration rate (eGFR) and sodium interact with cardiac cachexia in predicting cardiac events50). Conversely, age, hypertension, cancer, and levels of albumin, BNP, eGFR, and sodium are associated with it in predicting all-cause death50). Moreover, in HF patients with cardiac cachexia, we established thresholds predictive of cardiac events to be eGFR of 59.9 mL/min per 1.73 m2), age of 83 years, and hemoglobin of 10.1 g/dL, respectively50).
Regarding modifiable non-cardiovascular comorbidities, bleeding risks should be evaluated, because mortality increases after bleeding events in patients with HF10). Hemorrhagic diathesis has been attracting attention in recent years, particularly in association with patients having coronary artery disease, and criteria for high bleeding risk were defined by the Academic Research Consortium for High Bleeding Risk (ARC-HBR)51,52). This ARC-HBR definition is widely used, and a simplified version is also available53). However, bleeding risk in patients with HF has not yet been fully investigated. To address this issue, we evaluated bleeding risk in patients with HF using the simplified ARC-HBR definition54). Among the major criteria of ACR-HBR definition, the use of anticoagulants was found in a notably high proportion (56.5%) of HF patients54). Severe chronic kidney disease and severe anemia are also found in many HF patients (Figure 3)54). Our observational study revealed that the proportion of HF patients classified as having high bleeding risk (HBR) by the ARC-HBR criteria (83.1%) was much higher than that of patients with coronary artery disease with HBR (approximately 40-50%)54-56). HF patients with HBR had a 2.8-times higher incidence of bleeding events54). These results underscore the importance of evaluating bleeding risk in patients with HF57). To modify bleeding risk and improve prognosis, comprehensive management including adjustment of antithrombotic therapy is crucial58,59).
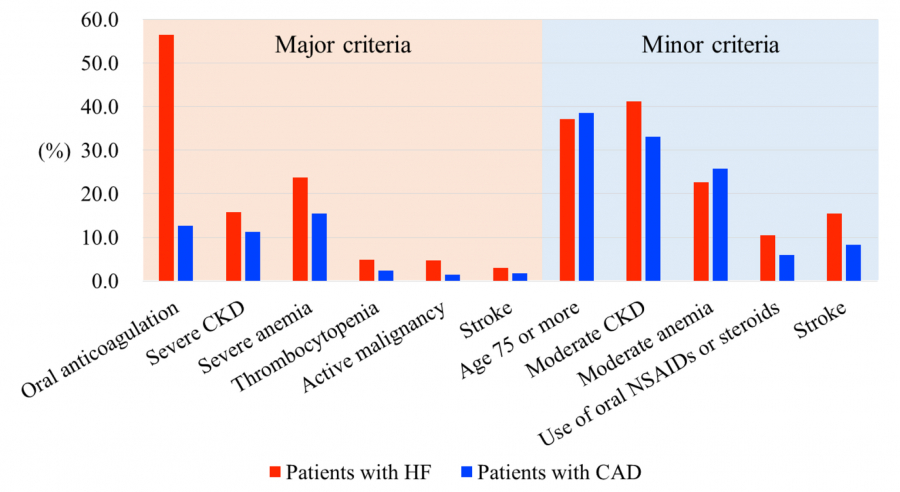
Fig. 3.
Comparison of the prevalence of the simplified ARC-HBR criteria in patients with HF and CAD in Japan
ARC-HBR, Academic Research Consortium for High Bleeding Risk; HF, heart failure; CAD, coronary artery disease; CKD, chronic kidney disease; NSAID, non-steroidal anti-inflammatory drug.
Adapted from Refs. 53 and 54.
Acknowledgements
The authors thank all of our colleagues for their assistance. The acquisition of data was supported by Ayumi Haneda, Akito Endo, Mari Hoshi, Manami Akimoto, Mimori Itami, Shiori Urayama, and Yuuichi Yokoyama from the Office for Diversity and Inclusion, Fukushima Medical University, Fukushima, Japan.
Conflict of Interest Disclosure
The authors declare no financial conflicts of interest pertaining to this review article.