Recommended exercise therapy for cancer survivors
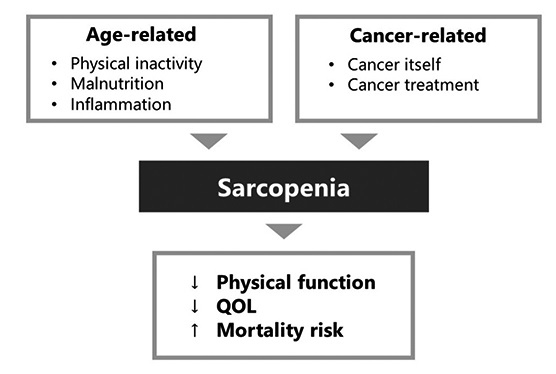
Exercise therapy is recommended for cancer patients, and has been reported to provide various benefits, such as improvements in physical function, QOL, and psychological well-being for cancer survivors after treatment (Figure 2)59-61). The exercise guidelines proposed by Campbell et al.60) state that engaging in exercise is safe for cancer survivors, and that inactivity should be avoided. Aerobic exercise and resistance training have been reported to contribute not only to improved physical function but also to the amelioration of anxiety, depression, fatigue, and health-related QOL in cancer survivors. In addition to the aforementioned physical benefits, the guidelines also address the potential benefits of exercise for treatment-related problems such as cardiotoxicity, peripheral neuropathy, cognitive dysfunction, nausea, and sexual dysfunction. Although the evidence is insufficient regarding the effectiveness of exercises for treatment-related problems, Campbell et al.60) recommend that inactivity should be reduced as much as possible. According to these guidelines, cancer survivors should engage in moderate-intensity activity for 150-300 minutes per week or high-intensity activity for 75-150 minutes per week. In addition, resistance training at least twice a week is recommended. The guidelines emphasize the importance of performing optimal exercises according to individual conditions and circumstances based on consultation with medical professionals before starting an exercise regimen. A study of adult cancer survivors reported that the percentage of those who met the recommended amount of physical activity ranged from 20% to 34%, and the percentage of those who adhered to resistance training two days per week was 12%62,63). In a study of breast cancer patients, 26% were engaged in guideline-equivalent activities 3 years after diagnosis64). However, many of the reports demonstrating the effects of exercise therapy targeted patients undergoing cancer treatment and cancer survivors without sarcopenia; there is a significant lack of studies focusing on survivors with sarcopenia following cancer treatment, both domestically and internationally. Therefore, the effect of adherence to exercise on cancer survivors with sarcopenia is unclear. However, in a report of hematologic malignancy patients undergoing chemotherapy, resistance training and aerobic exercise at an intensity equivalent to the Borg scale 13 at a frequency of once a day six times a week, resulted in a 95% adherence rate, even among patients with sarcopenia65). Moreover, in a study of cancer patients before surgery or during chemotherapy, whose population includes sarcopenic patients, resistance training and aerobic exercise improve physical function and skeletal muscle mass. In addition, the percentage of sarcopenia reversal has been reported to be approximately 20-30%. Furthermore, adherence to exercise has been reported to be around 50-85%66). Thus, high adherence to exercise has been reported even during periods when treatment-related adverse events are likely to occur, and similar or better exercise feasibility is expected in cancer survivors who have completed treatment. A report on exercise for breast cancer survivors, some of whom had sarcopenia obesity, reported an exercise adherence of 95%, resulting in improvement of body composition67). However, there are few studies on cancer survivors with sarcopenia, and the effects of exercise on such individuals have yet to be elucidated. Although increased exercise and physical activity are recommended, the existence of inadequate evidence between treatment-related side effects and the benefits of exercise is an issue that should be investigated by future studies.
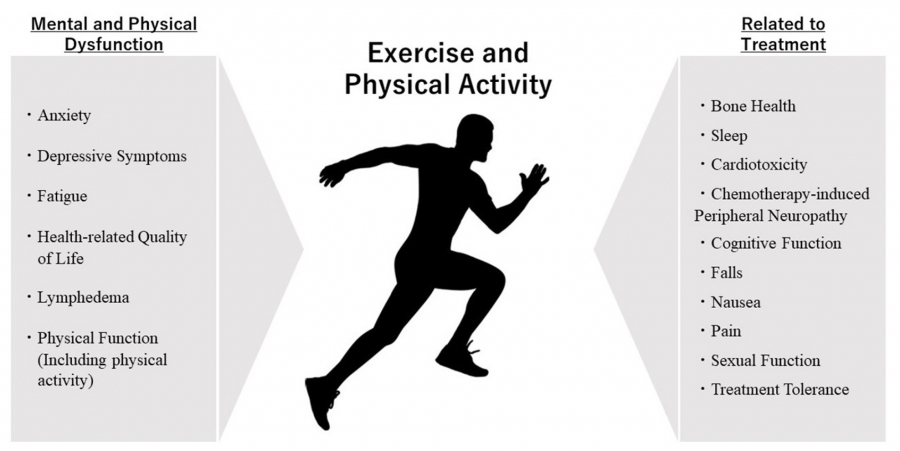
Fig. 2.
Benefits associated with exercise for cancer survivors
A Multimodal approach for cancer survivors
It is considered important to improve sarcopenia through nutritional therapy, exercise therapy, and physical activity66). In Japan, an oral ghrelin mimetic agent, anamorelin, has been developed as a therapeutic drug for cancer cachexia. This drug has been shown to prevent weight loss in patients with lung or gastrointestinal cancers68,69). Reports from Japan and other countries have suggested that a multimodal approach combining this medication with exercise, physical activity, and nutritional therapy maintains and improves body composition, physical function, and QOL70-73). Seemingly, this multimodal intervention requires multidisciplinary collaboration, and may raise concerns about feasibility and compliance. However, Naito et al71). reported that both nutritional and exercise interventions in elderly patients with advanced pancreatic and non-small-cell lung cancer showed high feasibility (> 90%) and no serious adverse events. Additionally, Liu et al.74) reported, in their study on elderly cancer survivors, that combining dietary guidance with exercise is effective for improving physical function; however, they concluded that further investigation is necessary to determine its impact on sarcopenia. A Cochrane review in 2014 that investigated exercise interventions for cancer cachexia patients reported that there was a lack of evidence to determine the safety and effectiveness of exercise, because no randomized controlled trials (RCTs) had met the inclusion criteria75). However, another Cochrane review in 2021 reported on four RCTs for head and neck cancer and lung cancer76). It is highly possible that these reports may be biased by factors such as masking of participants, personnel, and outcome assessors; thus, the efficacy, tolerability, and safety of exercise for cancer cachexia patients are still unclear, warranting more high-quality, well-designed RCTs in the future. While studies on multimodal interventions during cancer treatment have demonstrated the importance of sarcopenia prevention, reports incorporating medications and exercise remain limited, warranting further research development in the future.
Trial of exercise intervention for cancer survivors
In recent years, there has been an increase in reports on high-intensity interval training (HIIT) for cancer survivors. A study implementing high-intensity training for postoperative lung cancer survivors demonstrated improvements not only in physical function but also in muscle mass and QOL compared to patients receiving standard postoperative care only. In the present study, patients aged ≤ 80 years exercised for 60 minutes per session at a frequency of 3 days per week, for 20 weeks. Intensity was set at 80-95% of maximal heart rate for endurance training and 6-12 repetition maximum for resistance training, with a reported exercise retention rate of approximately 88% for 20 weeks77). In Japan, HIIT using smartphone-based support was conducted for breast cancer survivors, resulting in improvements in cardiorespiratory function and lower limb muscle strength78,79). This home-based program, indicated for breast cancer survivors aged 20–59 years, did not show significant improvement in QOL, but it achieved an adherence rate of 86% and did not result in serious side effects. The exercise program consisted of 6 weeks’ home exercise support using exercise counseling plus exercise instruction (six sessions per week, 30 minutes per session), 12 weeks of ICT intervention using personalized emails (one session per week) and an exercise application. Participants were encouraged to perform high-intensity body weight exercises set to increase in intensity each week, with one 10-minute training session three times per week for 12 weeks. The specific intensity was set at three levels of load according to cardiorespiratory fitness (VO2peak) at week 0, and was set to progressively increase fitness according to the individual’s fitness levels. The findings in these studies suggest that although consistent data on its effects on cancer survivors are not yet available, HIIT may provide both physical benefits and improved QOL to cancer survivors after treatment, and its continuation rates are noteworthy. Nevertheless, it should be noted that engaging in high-intensity workouts poses a potential risk of excessive exercise. It is important to remember that, to the best of our knowledge, no serious side effects associated with exercise interventions provided have been reported. In particular, if a study focuses on patients with reduced physical function, such as those with sarcopenia, it is even more important to receive expert advice regarding exercise load and physical condition management.
The use of smartphones to support intervention methods, as illustrated in the aforementioned HIIT, has been gaining in popularity. Interventions such as these using smartphones and other devices are referred to as mHealth. mHealth is a health and medical service that utilizes cell phones, applications, wearable monitoring devices, and other devices that can communicate and collaborate with each other. Onyeaka et al.80) found that cancer survivors use mHealth, via the use of health applications and wearable devices, at a similar rate to non-cancer patients (health applications, about 50%; wearable devices, 22%). Many cancer survivors have reported a desire to share information with their health care providers via mHealth. In addition, survivors who use health applications are more likely to meet the recommended vegetable intake and exercise regularly. They also reported that using mHealth not only improves physical function and physical activity, but also helps improve QOL, cognitive function, and fatigue81-83). Furthermore, combining mHealth with rehabilitation has been shown to increase the benefits of exercise82,83). Thus, mHealth could offer benefits to individuals recovering from sarcopenia, as it helps the management of both exercise and dietary habits, which are two key components in the effective treatment of this disorder. Such reports on mHealth have been reported in the U.S. and Spain, not only for middle-age cancer survivors but also for those aged ≥ 65 years. However, there are also concerns regarding the challenges of low adaptation of applications and wearable devices in the older population80-83).
Although none of the studies mentioned in this section involved post-treatment cancer survivors with sarcopenia, programs to improve skeletal muscle mass and physical function in cancer survivors have been reported, and innovative programs to prevent and improve sarcopenia should be explored in the future.
Problems and exercises related to sarcopenia
The effectiveness of exercise therapy has been reported with regard to issues related to sarcopenia, such as obesity and CVD risk. A study investigating exercise intervention targeting post-treatment breast cancer patients with obesity (including sarcopenic obesity) reported an increase in skeletal muscle mass over a 16-week period through aerobic exercise and resistance training, as well as improvements in biomarkers such as insulin, IGF-1, leptin, and adiponectin67). A study on obese breast cancer survivors also reported extensive benefits of exercise, which encompass improvements in physical function, bone health, QOL, cardiorespiratory function, and muscle strength84). Regarding CVD risks, the American Heart Association has introduced the concept of ‘cardio-oncology rehabilitation’ (CORE). By integrating elements of cardiac rehabilitation into cancer rehabilitation, CORE aims to enhance cardiorespiratory function and reduce CVD risks in cancer survivors. Reports from various countries have indicated that exercise therapy for cancer survivors leads to improved cardiorespiratory function 85-88), suggesting that exercise therapy may potentially mitigate CVD risk. Although exercises such as resistance training, aerobic exercise, and inspiratory muscle training have been reported to result in such risk-reducing effects89). there is no clear consensus on which type of exercise is most effective. Furthermore, to what extent sarcopenia affects CVD risk has not yet been definitively established. Most reports on the relationship between obesity and CVD risk come from overseas studies, and research into these aspects has been limited in Japan.
Sarcopenia has been shown to be clearly detrimental to cancer survivors during and after treatment; in a study of resected non-small cell lung cancer patients in Japan, Kawaguchi et al. reported that patients with sarcopenia had a higher recurrence rate than those without sarcopenia90). Although exercise therapy for cancer survivors is recommended and clearly provides a variety of health benefits, there is still a lack of research on sarcopenic cancer survivors. Recently, it has been suggested that skeletal muscle is involved not only in sarcopenia, but also in immune function, and that exercise and physical activity both support immune function and improve neurotrophic function, NK-cell cytotoxicity, and vaccine responses91). It has also become clear that exercise therapy has a positive effect on the immune system in cancer survivors, in addition to the improvement of physical function and the aforementioned effects. Specifically, it has been shown that exercise therapy in cancer patients reduces inflammatory cytokines such as interleukin-6 and tumor necrosis factor-α, which may lead to a reduction in fatigue92-94).
It is clear that further investigation should be conducted to determine the outcome of cancer survivors with sarcopenia after exercise therapy. While there are few overseas studies on exercise therapy for post-treatment cancer survivors, Japanese research significantly lags in this area. As the number of post-treatment cancer survivors is increasing in Japan, further research on the subject is essential and urgent.