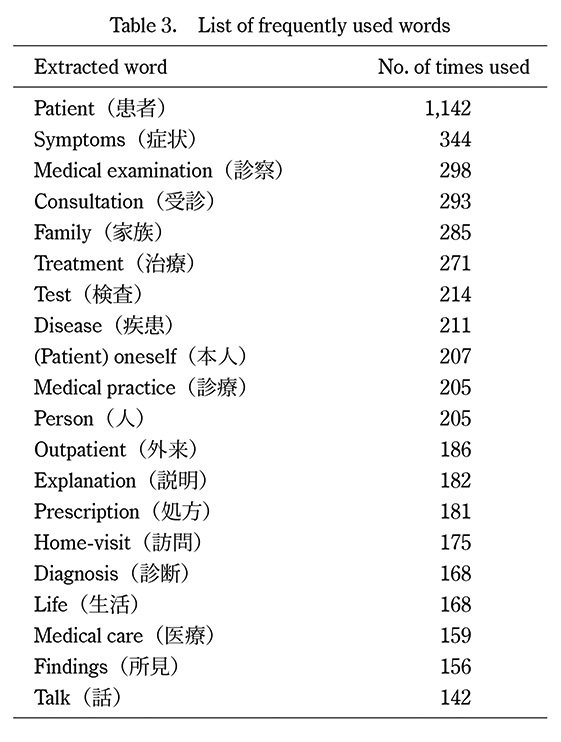
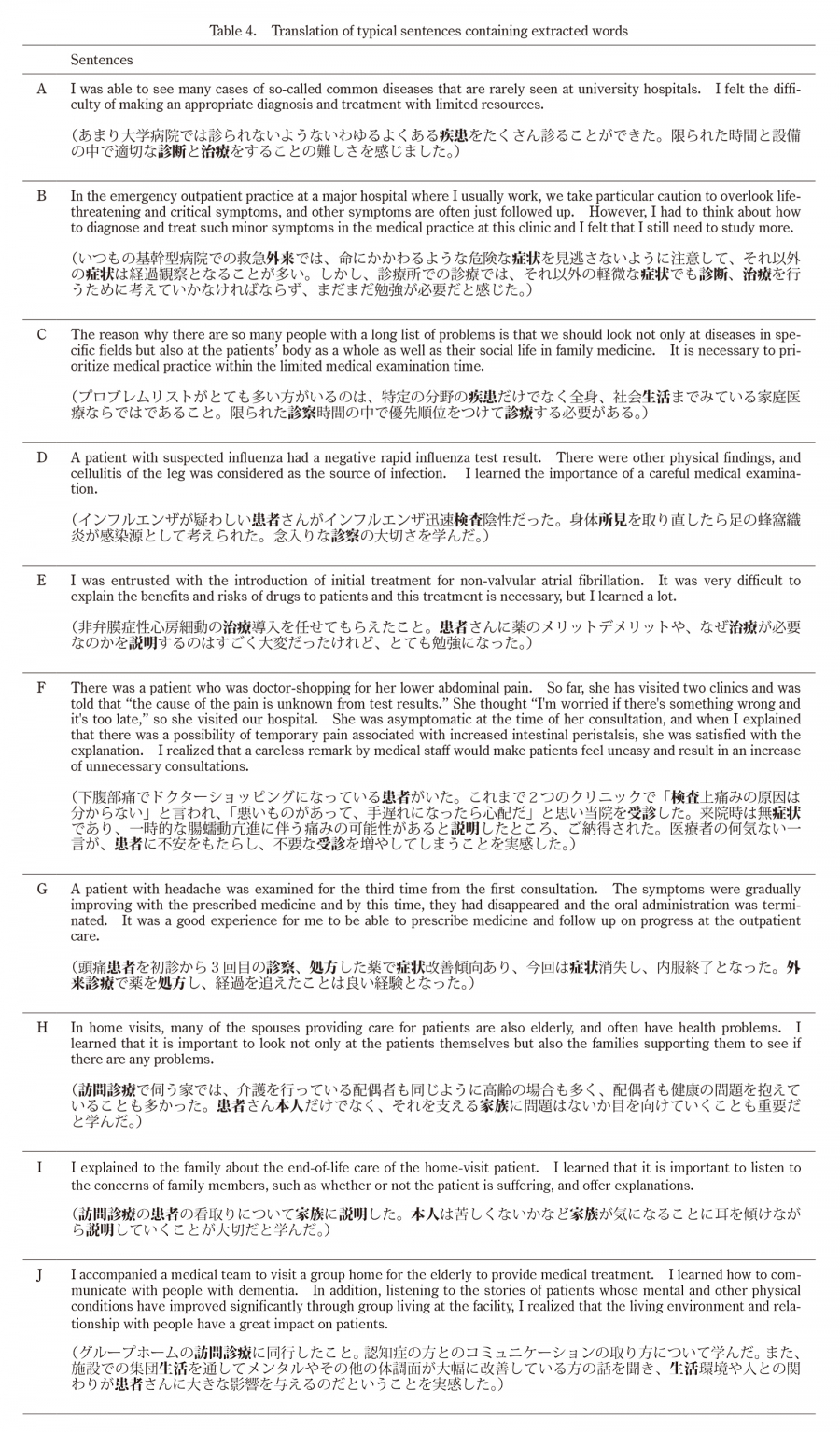
The top 20 most frequent words that appeared in sentences referring to clinical ability included “symptoms,” “medical examination,” “consultation,” “treatment,” “test, “disease,” “outpatient,” “explanation,” “prescription,” “diagnosis,” and “findings.” (see typical sentences A, B, C, D, E, F, and G in Table 4). In our previous study, which included the same participants as in this study, post self-evaluation of items related to clinical ability also increased compared to pre self-evaluation of GP/FM training8). By analyzing the reflective reports, we found that the reason was due to the GP/FM training complementing their previous training at core hospitals (such as university hospitals) (see typical sentences A, B, and C in Table 4) and that they were able to participate in and independently perform medical practice during the training (see typical sentences D, E, F, and G). Previous studies from other countries have reported that GP/FM training provides knowledge and skills that cannot be acquired in departmental training at hospitals13,14). Other studies have reported that the biggest difference in the learning environment between other hospital department training and GP/FM training is the increased responsibility that individual junior residents have regarding patient care; this greater responsibility further motivates the junior residents in their studies14,15).
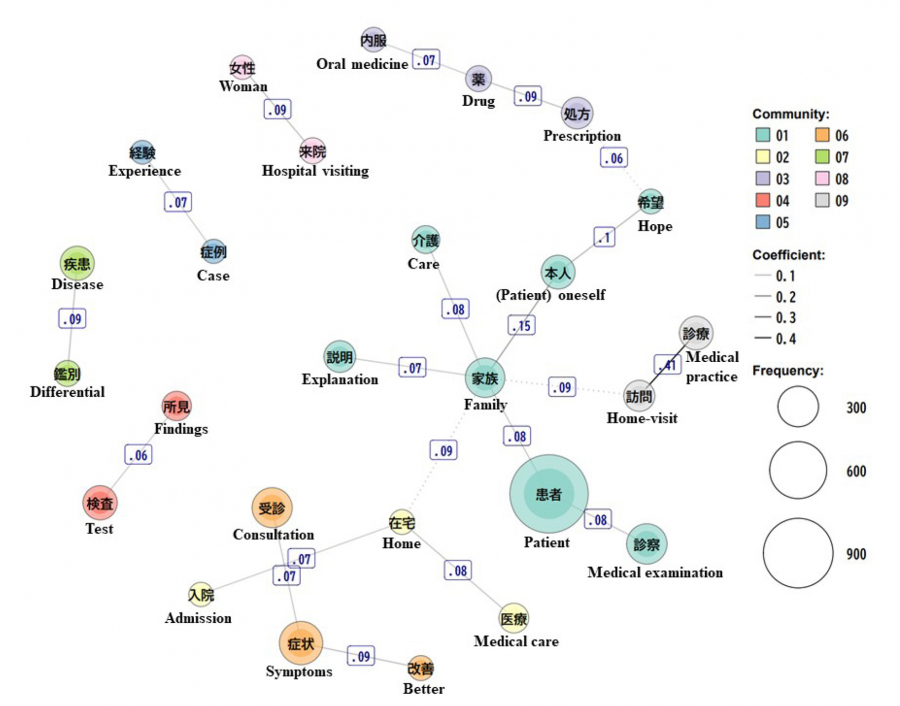
It is noteworthy that the second strongest co-occurrence relationship was found between “family” and “(patient) oneself” from the co-occurrence network map. This suggests that junior residents learned a significant amount not only about patient care but also about family-oriented care (see typical sentences H and I in Table 4). In our aforementioned study, post self-evaluation of items related to the care for patient’s family also increased compared to pre self-evaluation of GP/FM training8). However, it was difficult to explore the learning of “not only the patient but also the family as the target of care”’ with the existing evaluation items; therefore, we suspected that this aspect could be explored by analyzing the reflective writing. Previous studies have shown that GP/FM training promotes greater understanding in junior residents regarding the impact of illnesses on the family members of patients, compared with training in other specialties16). In another previous study we conducted that analyzed the reflective writing of GP/FM clerkships of fifth-year medical students at Fukushima Medical University, “family” was the fifth most frequently used word, suggesting that the participants learned a lot about family-oriented care17). On the other hand, a study reported by another Japanese university showed that the top six frequent words used in the reflective reports of the fifth-year medical students attending community medicine clerkship was “patient,” “systemic treatment,” “locale,” “hospital,” “care,” and “training” but “family” was not included10). This suggests that substantial learning about family-oriented care may be a characteristic of GP/FM training and clerkship which, therefore, can be or should be included in learning objectives of GP/FM training, if it is not the primary objective.
“Home visit,” “medical practice,” and “life” appeared most frequently in the descriptions related to understanding a patient’s psychosocial background (see typical sentence J in Table 4). In the co-occurrence network map, the strongest relationship was found between “home visit” and “medical practice” because the two words are often used as a compound word “home-visit medical practice” (訪問診療). In our previous study, post self-evaluation of items related to psychosocial background also increased compared to pre self-evaluation of GP/FM training8). Previous studies from other countries have also reported that home visits are the starting point for understanding social and economic factors related to holistic medical care and patient’s clinical conditions18). Unlike outpatient care, home visit training involves actual visits to patient’s home where junior residents can learn about patient’s psychosocial background by observing their living environment and daily life. Among the top 20 frequently occurring words, “patient,” “person,” “medical care,” and “talk” were used extensively in a rather general context and it was difficult to find a characteristic meaning. In the co-occurrence network map, the Jaccard coefficient, excluding “home visit” and “medical practice”, “family” and “(patient) oneself”, was 0.1 or less. This is probably due to the amount of data. In this study, the total number of sentences was 4,903 and the total number of words was 116,279. We reported a study of medical students using a method similar to the present study17). In the previous study, the total number of sentences was 321 and the total number of words was 10,627, and the Jaccard coefficients of the co-occurrence network map were all 0.1 or higher. Therefore, it was suggested that co-occurrence was difficult to find in this study due to the large amount of data.
This study has several limitations. The first limitation is that the superiority of GP/FM training over other types of postgraduate training is not yet verified. Although there have been few prior studies comparing GP/FM training and other training, GP/FM training was reportedly equal to or better than other types of training in terms of education quality, acquisition of clinical skills, social support, and role independence14). Second, because the text data are student-reported outcomes, there might have been some self-reporting bias. It is possible that the junior residents made positive statements out of gratitude and/or consideration for the family doctors supervising them. Third, although it is possible to explore learning using text mining, it is not possible to accurately evaluate it.