There is a lack of palliative care provision in the Japanese community. This can be verified by the fact that only 24% of cancer patients who died in Japan between April 2009 and May 2010 used specialized palliative care services, and most services were provided only to hospitalized patients1). Consequently, a basic policy regarding improving the social environment by enhancing cancer care and support was introduced in 2018. This policy calls for the establishment of a community support system in close collaboration with local and national governments, medical care institutions, schools, and private organizations to compensate for the lack of palliative care service provision in the community. This policy has been termed “The Future Direction of the 3rd-term Comprehensive 10-year Cancer Control Strategy.”2)
Community healthcare professionals need to acquire palliative care knowledge, skills, attitudes, and behaviors. Although palliative care education is being developed and delivered internationally, there are indications that patients are inappropriately cared for by physicians with inadequate training3). In Japan, palliative care education for physicians has been promoted as a matter of policy. The Cancer Control Act4) of 2007 promotes the early discovery of cancer, including the distribution of cancer treatment and research. It is part of “the Basic Plan to Promote Cancer Control Programs”5) and includes goals such as “Conduct basic training on palliative care for all doctors and promotion of cancer registration.” In 2008, “the Palliative Care Emphasis Program on Symptom Management and Assessment for Continuous Medical Education (PEACE)” was launched nationwide to provide basic palliative care training for physicians involved in cancer treatment. PEACE has been credited with improving physicians’ knowledge and palliative care practice and difficulties with palliative care in designated cancer hospitals6,7). However, these are mainly for physicians working in hospitals and not for community healthcare professionals.
Community palliative care training is in its developmental stages. “The Outreach Palliative Care Trial of the Integrated Regional Model (OPTIM)” was conducted as a multiple-intervention study in four regions of Japan from 2008 to 2010. The study reported improvements in the local physicians’ knowledge of palliative care and their perceptions of difficulties8-10). However, it is not clear which training methods will improve the ability of individual community healthcare professionals to practice community palliative care. It is important to identify how community healthcare professionals apply their knowledge to practice and the training methods that influence practice to achieve high-quality palliative care delivery in the community.
Family physicians (FPs) are expected to be one of the providers of community palliative care, even though they are not physicians specializing in palliative care. FPs are primary health care (PHC)12) professionals, and Internationally, community-oriented palliative care is referred to as primary palliative care and is provided according to PHC principles13-15). Murray suggested that with adequate training, resources, and professional support, FPs can provide end-of-life care for most patients13). A previous study of FPs in Taiwan found that 18.8% had experience with palliative care, and approximately 40% were engaged in home visits16,17). A study of 52 Belgian FPs found that almost all had a receptive attitude toward palliative care; however, they were uncertain about their role in decision-making and negotiation, suggesting a lack of knowledge regarding palliative medicine18). In a survey of 516 FPs in the UK, respondents felt that FPs play an important role in palliative care, indicating a need for training and professional development to enhance their palliative care knowledge, skills, and attitudes19). In Europe, FPs are trained to provide palliative care during the early stages of a disease20,21).
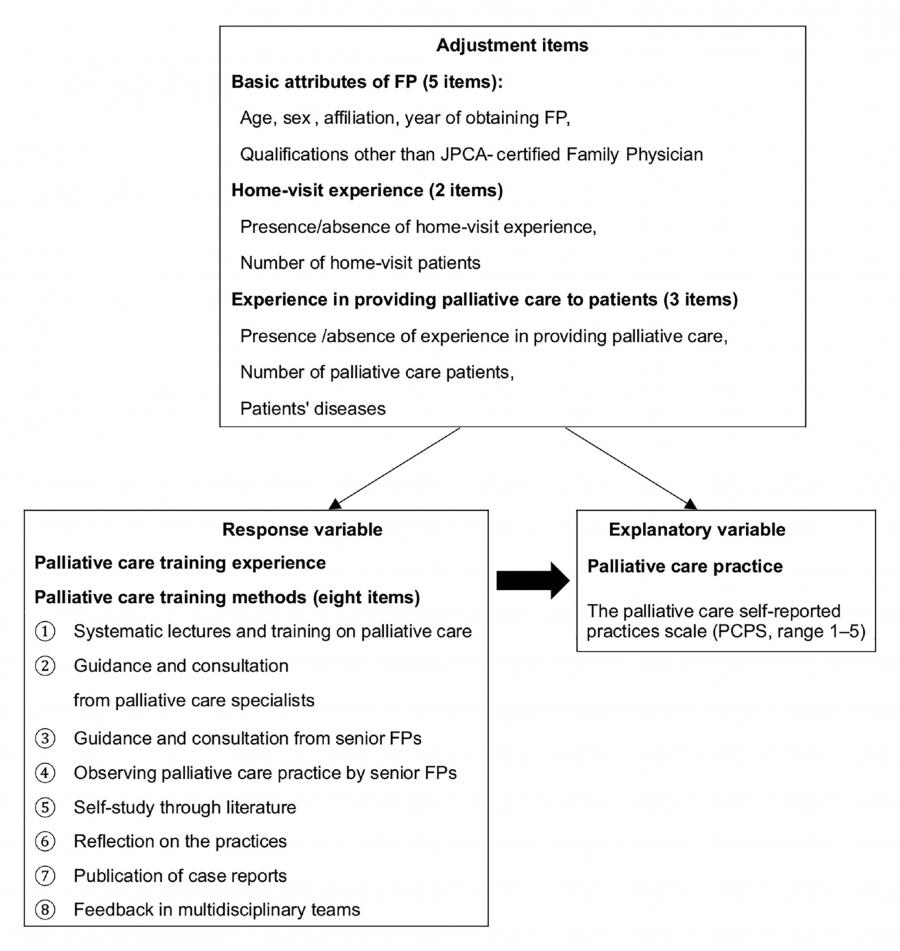
FPs contribute to community palliative care but lack long-term professional training in this area. It is unclear what training methods help them acquire community palliative care capacity. This study investigated the training methods used by certified FPs to enhance their professional development in palliative care and to determine the relationship between these methods and palliative care practice. The results will contribute to the development of training methods for physicians from diverse disciplines, as well as nurses and other community healthcare professionals, enabling them to acquire the necessary competencies required for community palliative care.