Background characteristics and biochemical parameters of patients
As shown in Table 1, refeeding methods were divided between oral nutrition (12 patients) and total enteral nutrition (6 patients). Patients who experienced a recurrence all selected OD, while younger children tended to select TPN, typically due to a refusal of oral intake or a fear of swallowing. The disease classifications, according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), included AN-R (12 patients), AN-BP (3 patients), and ARFID (3 patients). The mean ages of the participants were 17.3 (range: 12-24) years in the OD group and 12.6 (range: 11-13) years in the TPN group. The OD group included patients with recurrence. The mean ages and heights at admission were significantly higher in the OD group than in the TPN group (p < 0.01 and p = 0.03, respectively). However, there was no significant difference in SD score (p = 0.35). The mean BMIs at admission were 12.8 (range: 11.1-15.6) kg/m2 in the OD group and 12.7 (range: 11.2-15.2) kg/m2 in the TPN group. When compared by SD score, the mean BMI-SDS was −5.20 (range:−8.70-−2.66) in the OD group, and that in the TPN group was −3.54 (range:−5.66-−2.34). However, there was no significant difference in body weight between the two groups. Moreover, there was no significant difference regarding duration from anorexia nervosa onset to admission and the rate of weight loss.
All the patients’ blood test results for blood count, electrolytes, and liver transaminase were within reference intervals at admission. The OD group had significantly lower serum p levels than the TPN group. However, none of the patients presented with serum p levels below the reference range. In both groups, total cholesterol (TC) and triglyceride (TG) levels at admission were within or above their respective reference ranges. FC level at admission did not significantly differ between the groups. In all patients, the free triiodothyronine (T3) value, which indicates malnutrition, was below the reference range. However, there were no significant differences between the two groups.
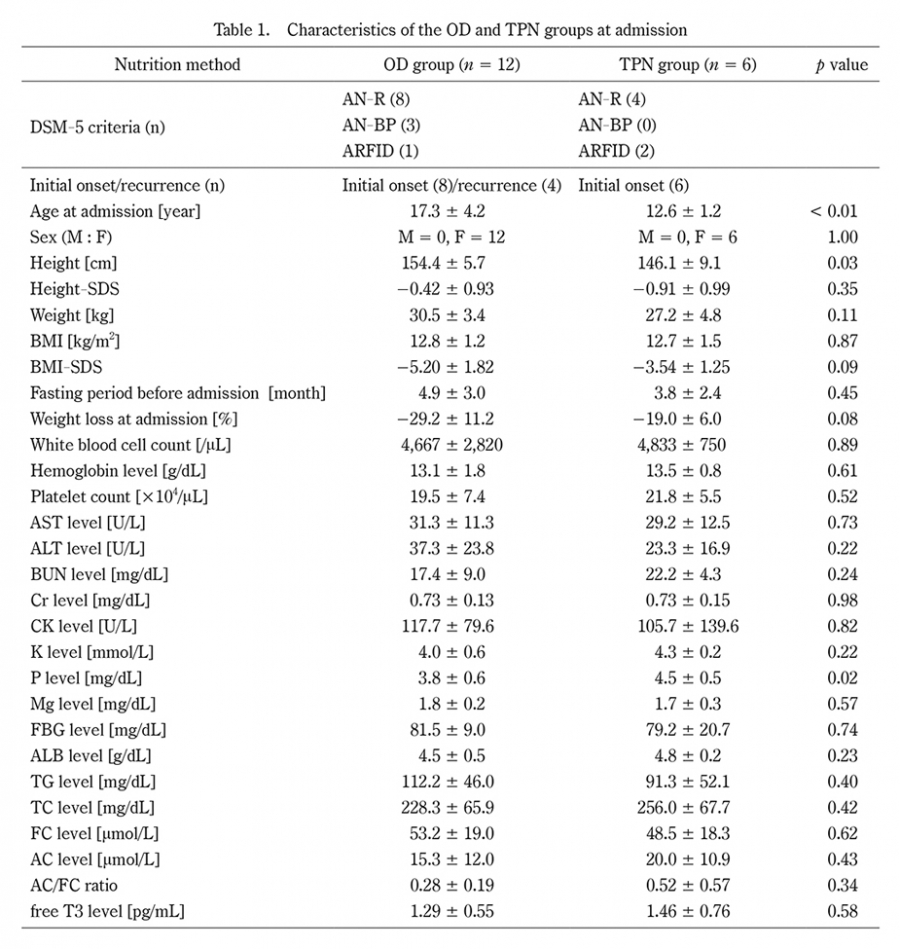
Table 1. Characteristics of the OD and TPN groups at admission
OD: oral diet, TPN: total parenteral nutrition, AN-R: anorexia nervosa restricting type, AN-BP: anorexia nervosa binge-eating/purging type, ARFID: avoidant/restrictive food intake disorder, BMI: body mass index, M ± SD: mean ± standard deviation, FBG: fasting blood glucose, TG: triglyceride, TC: total cholesterol, FC: free carnitine, AC: acylcarnitine, free T3: free triiodothyronine,
Data were expressed as M ± SD, with p < 0.05 indicative of a significant difference between the OD and TPN groups.
Metabolic parameters before and after the start of refeeding
Figure 1 shows the number of patients in the OD group and the TPN group one month after refeeding. Patients who developed refeeding syndrome were excluded. As shown in Table 2, the total energy dose per body weight was significantly higher in the OD group (n = 11) than in the TPN group (n = 5) at the start of refeeding (32.1 kcal/kg vs 8.8 kcal/kg) and 1 week after admission (36.3 kcal/kg vs 19.8 kcal/kg), but no significant difference was shown at 2 weeks (45.6 kcal/kg vs 35.5 kcal/kg) or at 4 weeks (51.0 kcal/kg vs 46.6 kcal/kg). Figure 2 shows changes in the total energy dose and the individual doses of each of the three nutrients (Fig. 2a), as well as and variations in heart rate and BMI (Fig. 2b), over a 1-month period after starting refeeding. The TPN group had significantly lower values for total energy dose, glucose, and protein than the OD group, both at admission and at 1 week after the start of refeeding. The values for total energy dose, glucose, and protein at 2 weeks did not show a significant difference (45.6 vs 35.5 kcal/kg, p = 0.08, 5.8 vs 6.3 kcal/kg, p = 0.60, and 2.2 vs 2.6 kcal/kg, p = 0.19). However, the glucose dose at 4 weeks was significantly higher in the TPN group than in the OD group (7.2 vs 9.9 kcal/kg, p = 0.03). The lipid dose at 4 weeks was significantly higher in the OD group than in the TPN group (1.4 vs 0.7 kcal/kg, p < 0.001), although the latter started receiving lipid preparations after 2 weeks of hospitalization. BMI-SDS did not significantly differ between the two groups during the entire refeeding process, although HR was significantly higher in the TPN group than the OD group at 4 weeks (61.2 vs 73.4, p = 0.02) (Fig. 2b).
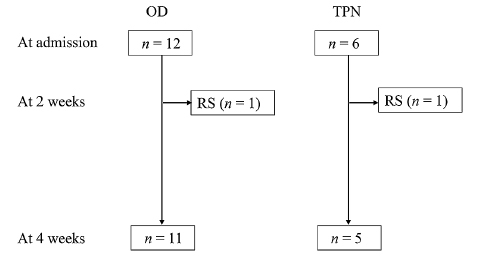
Fig. 1. Flowchart of patient enrollment and division into two nutrition methods
One patient in each group developed refeeding syndrome at day 11 of hospitalization; they were excluded from the evaluation. Neither presented with laboratory findings indicative of lipid metabolism. Nevertheless, the condition of these patients improved with intensive care.
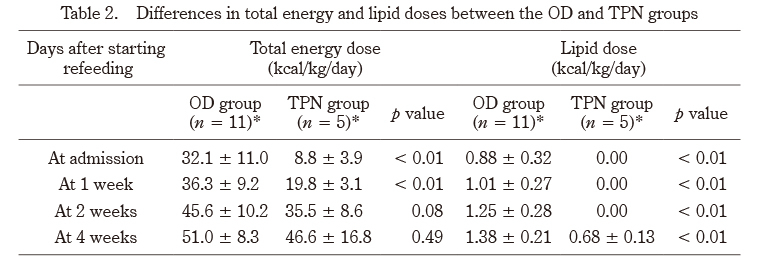
Table 2. Differences in total energy and lipid doses between the OD and TPN groups
OD: oral diet, TPN: total parenteral nutrition *Patients with refeeding syndrome were excluded.
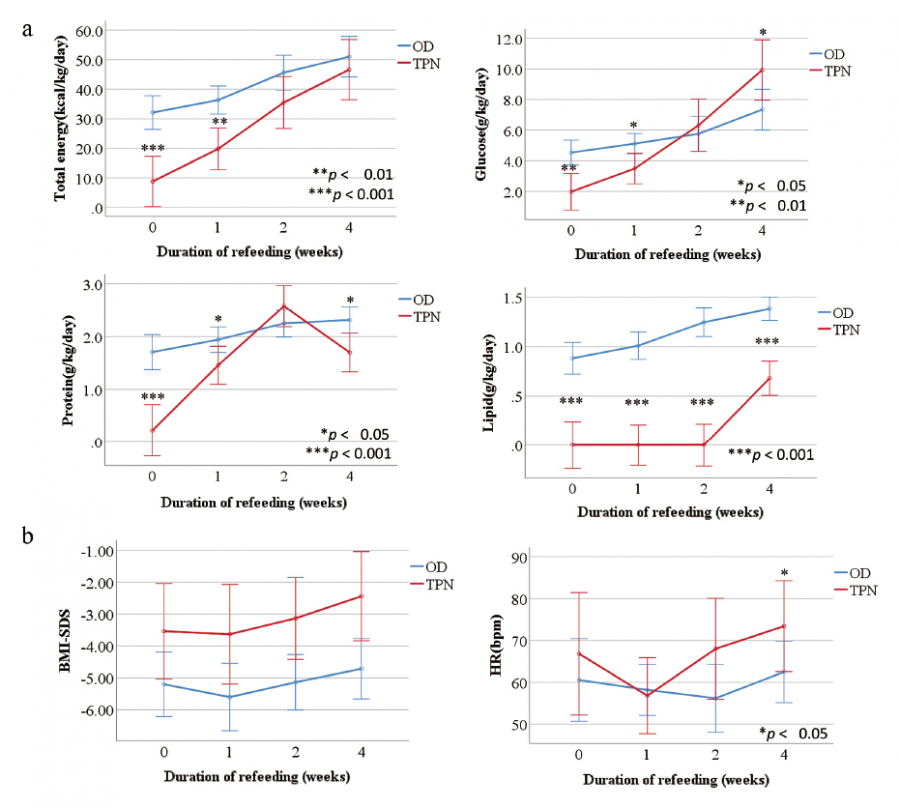
Fig. 2. Changes in the total energy dose, doses of three major nutrients, BMI, and HR
a. Changes in the total energy dose and doses of glucose, protein, and lipid. Patients in the TPN group initially had lower energy and glucose/protein doses than those in the OD group, but their glucose level sharply increased from week 2 to week 4 while that of the OD group patients showed a gradual and constant increase. This is likely associated with the initiation of lipid administration to the TPN group at 2 weeks from admission.
b. Changes in body mass index and heart rate over 4 weeks. Except for the HR at 1 week, there was no significant difference between the two groups.
BMI, body mass index;HR, heart rate;bpm, beats per minute.
Values are presented as mean ± SD for oral diet (n = 11) and total parenteral nutrition (n = 5). Significance values:*p < 0.05, **p < 0.01, ***p < 0.001. OD, oral diet;TPN, total parenteral nutrition.
Blood biochemical factors at 2 weeks after the start of refeeding
Table 3 shows the general blood analysis results of the OD and TPN groups. The OD group had a significantly lower serum P level than the TPN group. However, none of the OD group patients presented with serum P levels below the reference range (2.5-4.5 mg/dL). The fasting blood glucose (FBG) and serum albumin (ALB) levels did not significantly differ between the OD and TPN groups. Nevertheless, the TPN group had significantly lower TG (92.3 vs 32.6 mg/dL, p < 0.01), TC level (214.9 vs 133 mg/dL, p < 0.01), and AC/FC ratio (0.18 vs 0.10, p = 0.04) than the OD group. Moreover, the FC and AC levels did not differ between the two groups. However, the values decreased in both groups from the pre-refeeding levels
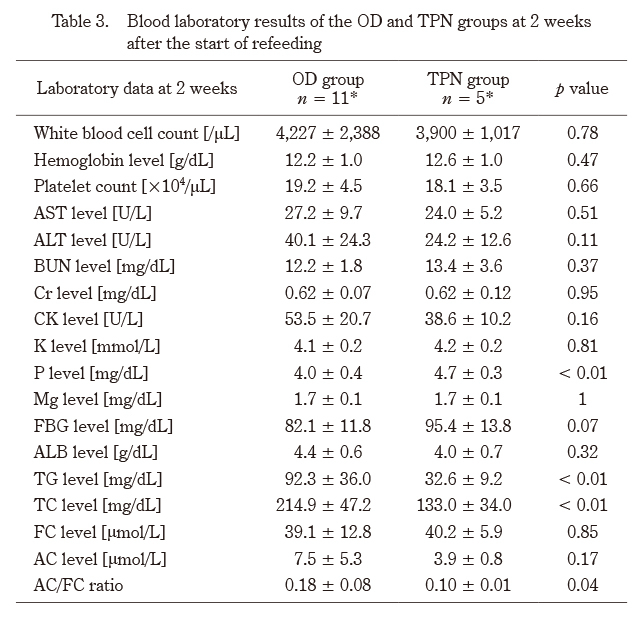
Table 3. Blood laboratory results of the OD and TPN groups at 2 weeks after the start of refeeding
OD: oral diet, TPN: total parenteral nutrition, M ± SD: mean ± standard deviation, FBG: fasting blood glucose, TG: triglyceride, TC: total cholesterol, FC: free carnitine, AC: acylcarnitine, free T3: free triiodothyronine
Data were expressed as M ± SD, with p < 0.05 indicative of a significant difference between the OD and TPN groups, excluding patients with refeeding syndrome. *Patients with refeeding syndrome were excluded.
Changes in lipid levels during the refeeding period
Figure 3 shows the changes in lipid levels over the refeeding process. At 2 weeks from the refeeding onset, the TPN group had significantly lower TC and TG levels than the OD group, although no significant differences were observed at 4 weeks. As for the FC level, two patients in the OD group and one in the TPN group had higher levels than reference range (36-74 µg/mL) at admission, which decreased to the reference range after refeeding started. On the other hand, three OD patients and one TPN group patient had lower FC levels than the reference range at admission, but after the start of refeeding, their values exceeded the reference range except one OD patient. The AC/FC ratio at admission was higher than the reference value (< 0.25) in five patients each in the OD group and TPN group. The AC/FC ratio of > 0.4, indicating carnitine deficiency, was observed in two patients in the OD group and one in the TPN group. At 2 and 4 weeks after the start of refeeding, the AC/FC ratio of both groups decreased from pre-treatment levels, and all patients had an AC/FC of < 0.4. In addition, the AC/FC ratio of the TPN group was significantly lower than that of the OD group (0.18 vs 0.10, p = 0.04 at 2 weeks; 0.15 vs 0.11, p < 0.01 at 4 weeks) (Fig. 3).
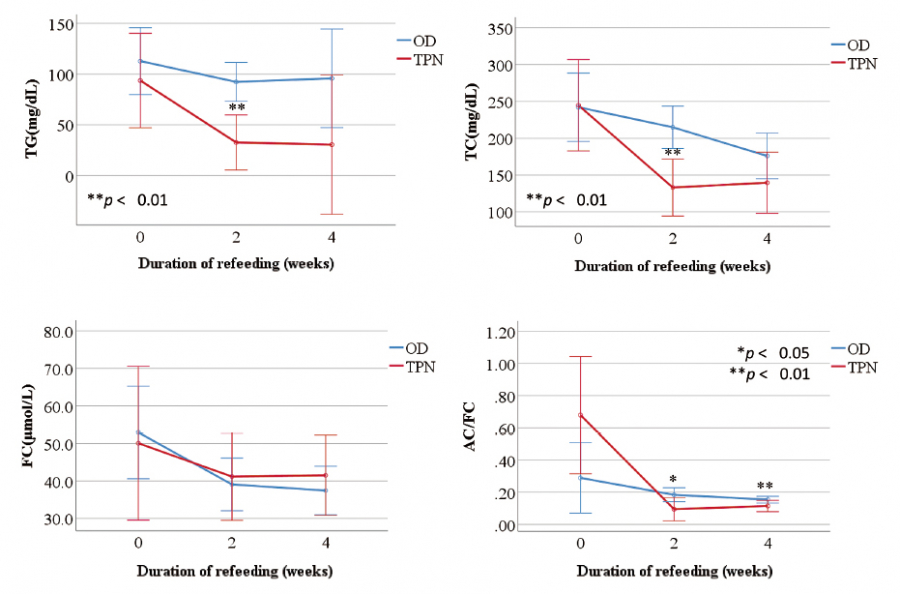
Fig. 3. Changes in lipid metabolism during refeeding
After two weeks of refeeding, the TPN group showed notably lower TC and TG levels compared to the OD group, although these differences were not significant at 4 weeks, as they had been at admission. The AC/FC ratio, an indicator of the carnitine level, was above the reference range in several patients on admission. However, after refeeding, all patients had an AC/FC of < 0.4.
The reference ranges in our hospital are TG 50-149 mg/dL, TC 150-199 mg/dL, FC 36-74 µg/mL, and AC/FC 0.25-0.4. TG, triglyceride; TC, total cholesterol; FC, free carnitine; AC, acyl carnitine; AC/FC, FC-to-AC ratio.

