Diffuse idiopathic skeletal hyperostosis (DISH) is characterized by bone hyperplasia of the skeletal system, particularly of the spine1). In this case, the spine becomes rigid, causing stress concentrations when exposed to external forces, with even minor trauma leading to a spinal cord injury2). DISH is a common indication for surgery, making patients susceptible to unstable spinal fractures due to anatomical features3).
The prevalence of DISH on computed tomography (CT) is as high as 27.2% in total, 38.7% in males, and 14.0% in females4). Moreover, the prevalence of DISH rises with increasing age5,6);therefore, this fracture is common, especially with increasing age.
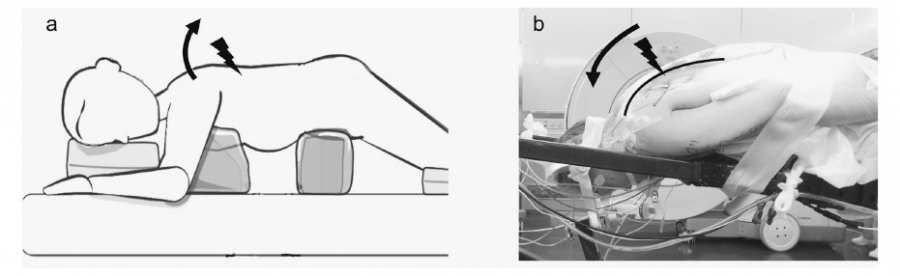
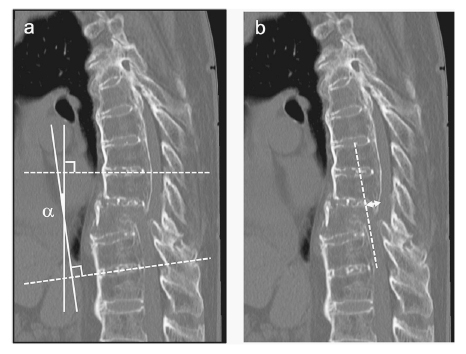
Patients with DISH often have thoracic kyphosis, resulting in loss of kyphosis or lordosis due to hyperextension injuries7). When the patient is placed in the prone position for posterior fixation with this fracture, extension forces are applied to the fracture site, exacerbating the displacement, and making the reduction challenging. If the anterior opening displacement remains after posterior fixation, the anterior column may be lacking, resulting in non-union and implant failure.
However, adding anterior fixation to avert such complications is highly invasive, increases the risk of complications, and is contraindicated in patients who may not handle the invasiveness7). Additionally, displacement of the fracture site may exacerbate neurological deficits. By performing preoperative reduction, we can achieve surgical goals with minimally invasive surgery comprising posterior fixation only. Moreover, indications for surgery could be extended, and a superior outcome could be observed. This also has the potential to prevent neurological exacerbations.
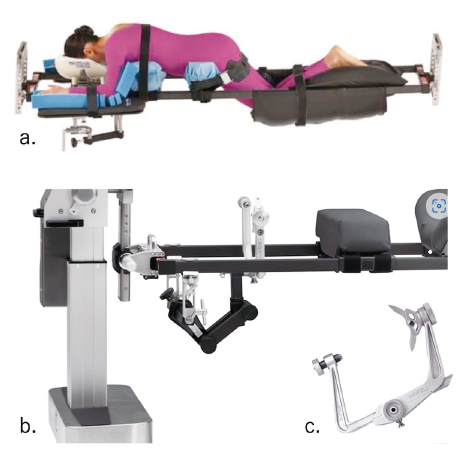
In this study, we establish a method for preventing displacement of the surgical position and approach repositioning using the skull clamp-assisted position (SAP) for thoracolumbar fractures with DISH. Additionally, we describe the technique and its precautions and report several cases treated with this method.