

Uterine leiomyomas are benign tumors that originate from the clonal proliferation of smooth muscle and affect 20%-60% of women of reproductive age 1,2). They rank as the most common solid tumors in premenopausal women3), with approximately half of the affected women being asymptomatic4). Symptoms associated with uterine leiomyomas include dysmenorrhea, hypermenorrhea, pelvic pressure, frequent urination, and sterility2). The growth of uterine leiomyomas depends on the expression of estrogen and progesterone receptors, suggesting that they may continue to grow even after menopause. Additionally, uterine leiomyomas can display several histological features attributed to degeneration, including a rare variant known as hydropic leiomyoma (HL). HL exhibits characteristic features, such as zonal distribution of edema, increased vascularity, and arrangement of tumor cells in nodules or cords5). Owing to its rarity, clinical features of HL, including its appearance on ultrasound and magnetic resonance imaging (MRI), remain scarce. In this report, we present a case of a premenopausal woman with HL that mimicked an ovarian tumor.
The content of research paper
Hydropic leiomyoma-like ovarian tumor: a case report
Tomoko Yamaguchi, Hyo Kyozuka, Yoshihiro Kochi, Fumihiro Ito, Hajime Odajima, Daisuke Suzuki, Yasuhisa Nomura
-
Tomoko Yamaguchi
Department of Obstetrics and Gynecology, Ohta Nisinouchi Hospital
-
Hyo Kyozuka
Department of Obstetrics and Gynecology, Ohta Nisinouchi Hospital
-
Yoshihiro Kochi
Department of Obstetrics and Gynecology, Ohta Nisinouchi Hospital
-
Fumihiro Ito
Department of Obstetrics and Gynecology, Ohta Nisinouchi Hospital
-
Hajime Odajima
Department of Pathology, Ohta Nisinouchi Hospital
-
Daisuke Suzuki
Department of Obstetrics and Gynecology, Ohta Nisinouchi Hospital
-
Yasuhisa Nomura
Department of Obstetrics and Gynecology, Ohta Nisinouchi Hospital
Introduction
Case presentation
A 49-year-old nulliparous Japanese woman presented to our hospital with a two-year history of abdominal distension. Ultrasonography indicated the presence of a large space-occupying lesion with a solid and cystic component (with a septum) extending from the lower part of the liver to the lower abdomen. The uterus showed continuous enlargement from the middle part with unclear boundaries, becoming cystic lesions in certain areas (Fig. 1). Therefore, it was challenging to differentiate between ovarian and uterine tumors, leading to suspicion of tumors originating from either the ovaries or the uterus.
The MRI scan of the pelvis revealed a poorly defined mass measuring 20 cm in diameter located in the posterior part of the uterus. The mass displayed a cystic component, with a solid component identified in the lower-middle portion of the mass. The T2-weighted image of the solid component showed heterogeneity, with a T2 hyperintense tumor observed within the interior of the solid component (Fig. 2a). Additionally, diffusion-weighted imaging (DWI) conducted with MRI showed a decrease in the diffusion-enhanced image in an area that could not rule out malignancy, along with a reduction in the Apparent Diffusion Coefficient’s (ADC) diffusion (Fig. 2b, 2c). However, the actual ADC values could not be obtained due to the precision limitations of the MRI equipment. Regarding the ovaries, it was challenging to confirm their intact status and age-appropriate appearance preoperatively via MRI. The patient’s serum cancer antigen CA-125 levels were elevated to 52.9 U/mL (normal range: 0 to 35 U/mL). Cytology of the uterine cervix and body showed no significant findings. Based on these findings, pelvic cancer, especially serous-type ovarian cancer, was suspected. We decided to perform a total abdominal hysterectomy and bilateral salpingo-oophorectomy. During the laparotomy, no ascites were noted, and there were no adhesions between the organs. Both ovaries were intact, and a cystic tumor measuring approximately 20 cm in continuity with a swollen fibroid was observed (Fig. 3A). Upon cutting open the excised uterus, serous fluid accumulation was identified in the cystic tumor (Fig. 3B). The pathological examination revealed a fibroid appearance corresponding to a gross white nodular area. Fibroids showed smooth muscle cell proliferation accompanied by various degenerative changes (Fig. 4A). There was no significant evidence of cellular atypia or increased mitotic activity in proliferating smooth muscle cells, indicating an appearance consistent with leiomyoma (Fig. 4B). The patient was discharged without any complications on the fourth day after surgery. Based on the gross intraoperative findings and pathological examination, the final diagnosis was hydropic leiomyoma. The CA-125 level had decreased to 6.9 U/mL one month after the surgery.
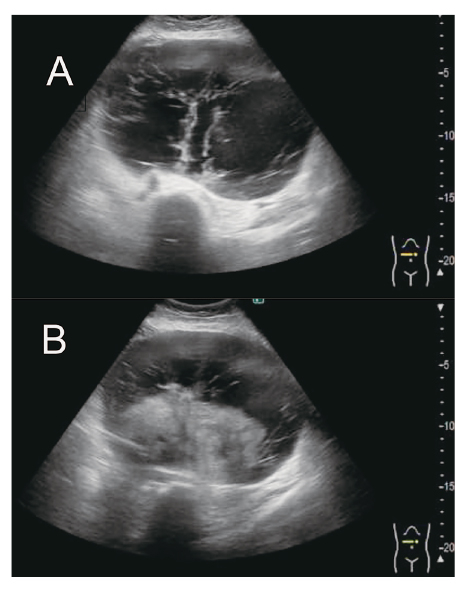
Fig. 1. Transabdominal ultrasound findings at the first visit.
A. A large space-occupying lesion with a congested area and a cystic region with septations is observed in the lower part of the liver to the lower abdomen.
B. The boundary of the uterus is unclear, and a solid area is continuously observed, which transitions into a cystic lesion from the middle. It is difficult to differentiate whether the lesion originates from the ovary or uterus.
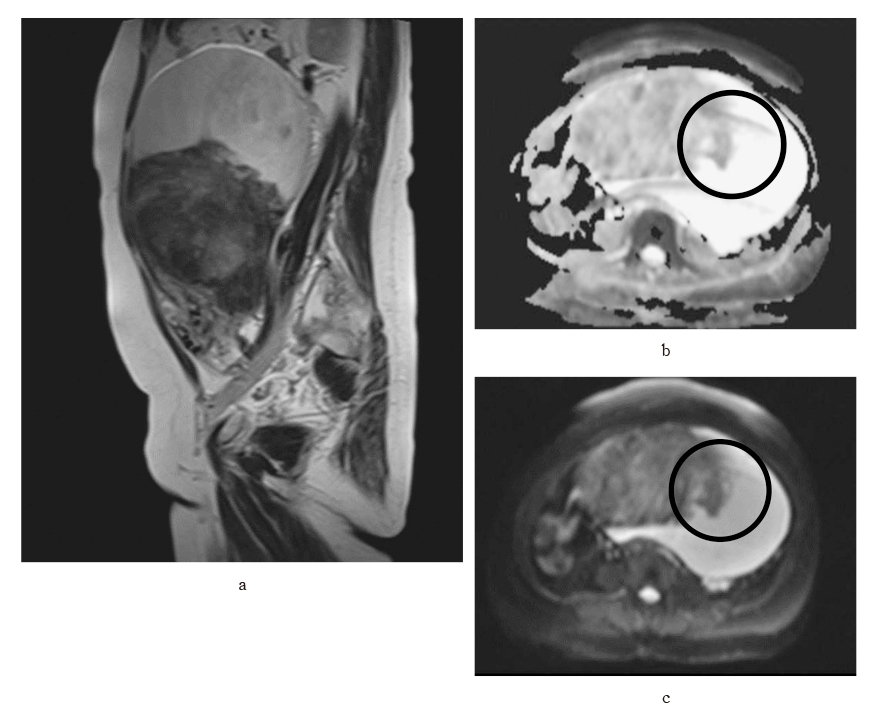
Fig. 2. MRI findings at the first visit.
a. The T2-weighted image of the solid component showed heterogeneity, with a T2 hyperintense tumor observed within the interior of the solid component.
b. In the diffusion-weighted imaging, we observed a decrease in the diffusion-enhanced image in an area (marked with a circle). This circled area shows papillary proliferation, which means we cannot rule out malignancy. (2b).
c. Additionally, there was a reduction in the Apparent Diffusion Coefficient’s diffusion (2c).
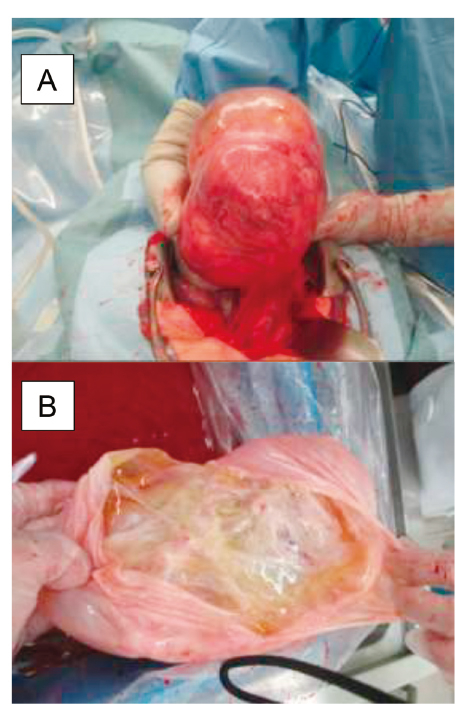
Fig. 3. Intraoperative findings.
A. We identified the tumor as a cyst that was continuous with the uterine serosa and noted that it was not adhered to the surrounding tissue.
B. When the cyst on the surface of the excised uterus was opened, it was filled with a transparent serous fluid component, and no solid part was macroscopically identified.
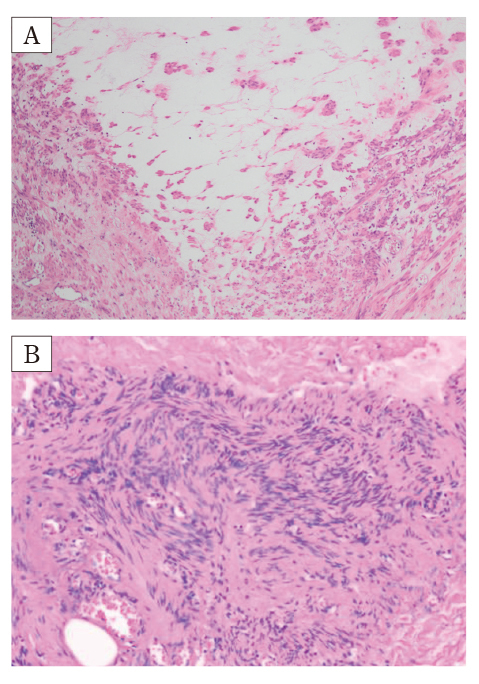
Fig. 4. Pathological findings.
On Hematoxylin and Eosin staining, the tumor showed proliferation of smooth muscle cells with various degenerative changes.
A. The excised uterine tissue exhibited membranous components composed of fibrous tissue and edematous interstitial elements, showing continuity with areas of marked edematous changes at the margins of the leiomyoma. This observation suggests that the highly degenerated parts of the leiomyoma underwent membranous detachment.
B. No remarkable atypia or mitotic figures were observed in the proliferating smooth muscle cells, which is consistent.
Discussion
Hydropic leiomyoma is a rare and distinct variant of uterine leiomyoma and is characterized by significant hydropic degeneration. This benign tumor originates from the smooth muscle cells of the uterus5). Owing to its infrequency, information on this condition is limited, and many aspects remain unexplored. Hydropic leiomyoma is characterized by watery edema and can sometimes resemble gynecological malignancies, rendering the distinction between them vital5).
In the present case, the elevated CA-125 level of 52.9 U/mL raised suspicions of an ovarian tumor. Previous studies have demonstrated that the levels of tumor markers, particularly CA-125, are generally elevated in patients with uterine leiomyomas. Elevated CA-125 levels are often observed in patients with uterine leiomyomas, especially those > 5 cm in size6). Therefore, CA-125 cannot be solely used to differentiate between ovarian tumors and uterine myomas > 5 cm in size.
Ultrasonography (US) is commonly used as the initial imaging modality to evaluate uterine leiomyomas7). The characteristic ultrasound appearance of a leiomyoma includes well-defined hypoechoic masses relative to the normal myometrium, with round or oval-shaped lesions exhibiting a whorled appearance. The uterine contour may be deformed due to the mass effect, with circumferential vascularity visible on color Doppler ultrasonography7). However, the clinical features of hydropic leiomyoma are not well understood. As hydropic leiomyoma is marked by watery edema, its ultrasound features may appear more heterogeneous than those of typical leiomyomas owing to the presence of cystic spaces and a complex appearance. However, similar to conventional leiomyomas, hydropic leiomyomas generally have well-defined margins owing to their benign nature.
MRI offers comprehensive information on the anatomy and characteristics of leiomyomas. Typical MRI features of leiomyomas include discrete, rounded, and well-circumscribed myometrial masses with homogeneous low-signal intensity on T1-weighted images and homogeneous low-to-intermediate signal intensity on T2-weighted images8). Previous imaging studies of hydropic leiomyomas have presented a variety of findings, ranging from well-demarcated uterine tumors to complex, multinodular masses that obscure the adnexa and occasionally displace nearby organs9-12). These images also reveal degenerative or cystic changes akin to malignant tumors, such as leiomyosarcoma13-16). Consequently, efforts have been directed towards using MRI to specifically differentiate whether a leiomyoma is malignant17,18). A recent study demonstrated that features such as lobulated borders, T2 dark areas, necrosis, hyperintensity of the tumor relative to the myometrium after contrast administration, central necrosis, a high signal on b1000 DWI, and an ADC value lower than 0.82×10 -3 mm2/s could assist in distinguishing atypical leiomyomas from leiomyosarcomas18). Furthermore, the combination of lobulated borders and central necrosis may aid in predicting malignant histology18). However, in our current case, where both the DWI and ADC showed a decrease, it was challenging to definitively differentiate between benign and malignant preoperatively or ascertain whether the tumor originated from the uterus or ovary. One feature useful for differentiating hydropic leiomyoma from malignant tumors is the “split fiber” sign19). This sign is identified by the presence of curvilinear T2 hypointense strands within the degenerated leiomyoma, which are separated by fluid accumulation and edema. While hydropic degeneration shows limited or poor enhancement post-contrast, malignancies typically exhibit variable enhancement. The “split fiber” sign, observable in T2-weighted images, helps in distinguishing between these conditions19).
It is crucial to acknowledge that hydropic leiomyomas can mimic malignant tumors on ultrasonography because of their atypical features. In conclusion, additional evaluations using other imaging techniques, such as MRI, or histopathological examination may be necessary to confirm the diagnosis and determine the appropriate management strategy. Given the difficulty in differentiating between degenerated leiomyoma and ovarian tumors, rapid histopathological diagnosis is considered important in clinical practice.
Acknowledgements
We express our gratitude to Dr. Tadanobu Tameda, who provided the radiological reading for this case.
Conflict of interest disclosure
The authors have no potential conflict of interest to declare.
Patient Consent
Informed consent was obtained from the patients for publication of this work.
Contributors
All authors were involved in the clinical care of the patient and contributed to the conception, drafting, review, and revision of the manuscript. All authors saw and approved the final version of the paper and take full responsibility for the work.
Funding
This work did not receive any specific grant from funding agencies.
Provenance and Peer Review
This case report was peer-reviewed.