

The functional prognosis after lower limb amputation largely depends on whether the heel can be preserved. In amputation of the lower limb, preserving the heel is a significant functional advantage. This is because preservation of the heel allows the weight to be carried without needing a prosthesis. Lisfranc amputation and Chopart amputation are surgical methods that are employed to preserve the heel, but Chopart amputation is considered to have a high risk of deformity, equinus, or varus, and result in poor function1,2). We here report a case in which Chopart amputation combined with tendon transfer and tendon lengthening was performed3), and the patient was able to walk independently with a foot prosthesis without deformity of the foot. We investigated walking speed and plantar pressure after Chopart amputation with and without a foot prosthesis.
The content of research paper
Investigation of walking speed and plantar pressure after chopart amputation
Kazuo Ouchi, Mari Sato, Yuki Kashiwabara, Mutsumi Shimazaki, Shoji Yabuki
-
Kazuo Ouchi
Department of Rehabilitation Medicine, School of Medicine, Fukushima Medical University
-
Mari Sato
Department of Rehabilitation Medicine, School of Medicine, Fukushima Medical University
-
Yuki Kashiwabara
Department of Rehabilitation Medicine, School of Medicine, Fukushima Medical University
-
Mutsumi Shimazaki
Department of Rehabilitation Medicine, School of Medicine, Fukushima Medical University
-
Shoji Yabuki
School of Health Sciences, Fukushima Medical University
Introduction
Case report
A 78-year-old man underwent vascular graft replacement for an abdominal aortic aneurysm, and then experienced right extremity thromboembolism, resulting in ischemic necrosis of the right forefoot. After the surgery, his general condition was poor, he was bedridden with a tracheotomy and an artificial respirator, and he had total dependence. However, his expression, comprehension, problem-solving. and memory were all sound. His functional independence measure (FIM) score was 20 points. Three months after surgery, the necrosis had spread to the middle part of the right foot, but since the patient’s general condition had improved, a right foot amputation was performed. Chopart amputation was performed because the necrosis extended to the central part of the sole. In the surgery, transfer of the tibialis anterior and peroneus brevis tendons, as well as Achilles tendon lengthening, were performed, taking into consideration the balance of the tendons, to prevent postoperative deformation.
For postoperative rehabilitation, to prevent deformity and protect the wound, the ankle joint was splinted for 3 weeks after surgery. From the day after surgery, the patient was able to move in a wheelchair without bearing weight on the affected limb. Two weeks after surgery, non-weight-bearing walking training was started. Three weeks after surgery, the splint was removed, and ankle joint range of motion training and full-weight walking training were started. Four weeks after surgery, he was able to walk with a walker. Five weeks after surgery, he was able to walk with a T-cane, and no varus or equinus deformity was observed (Figure 1). Active dorsiflexion and plantar flexion of the ankle were possible, and the range of motion was 5 degrees dorsiflexion and 10 degrees plantar flexion. The patient was able to stand and walk without a prosthesis with a heel load. However, he was unable to push off the ground and his right foot dragged when he walked forward. Therefore, a foot prosthesis was made (Figures 2-A and B) and attached 6 weeks after surgery (Figures 3-A and B). The foot prosthesis features a belt-type rubber tip and a 10 mm-thick sole, which is designed to attach the rubber tip to the foot. Due to the absence of equinus deformity, the posterior heel and anterior part of the amputation edge had the same height. The tip and sole are both made of rubber, the inside of the midfoot is made of sponge, and the surface is made of leather. As a result, the patient was able to push off the ground and was no longer limping while wearing the foot prosthesis. Moreover, he was able to walk 1 km while using a cane, as well as get on and off a bus independently.
Six years after surgery, at the age of 85 years, the patient's walking ability was stable, and he was able to perform his daily activities independently. Given this long-term stability, we conducted a comprehensive assessment of his walking ability. We measured walking speed and plantar pressure using a 10-m walking test, performed twice; once with and once without a prosthesis. During the test, the patient used a T-cane both with and without a prosthesis. The patient’s walking speed increased from 0.6 m/s without the prosthesis to 0.8 m/s with it; an increase of 33%. The stride length increased from 33 cm without the prosthesis to 50 cm with the prosthesis. The number of steps decreased from 30 steps without the prosthesis to 20 steps with the prosthesis.
The plantar pressure while walking was measured using an insole-type pressure distribution sensor (Pedar-X;Novel gmbh, Germany) (Figure 4). This device has 99 segmental sensors placed in the insole. The pressure was measured 6 years after surgery, when the patient was aged 85 years, using a T-cane with and without the prosthesis. A sheet sensor was inserted between the shoe and the foot, and another was inserted between the shoe and the prosthesis. Measurement was conducted three times, each time including five steps. The measurement with the least data variability was used, and the mean maximum pressure was calculated. The pressure at the amputation stump was the average of seven sites in the most distal row (Figure 5, sixth row counting from the rear, the row indicated by the red arrows) where the values were obtained. The same sites were used to calculate the amputation site pressure with a prosthesis. Figure 5-A shows a plantar pressure map without the prosthesis and Figure 5-B shows the same map with the prosthesis. At the amputation stump, the plantar pressure was 129.3 N/cm2 on average without the foot prosthesis but decreased by 59% to 51.6 N/cm2 on average with the foot prosthesis. Regarding the plantar pressure of the non-amputated foot, the pressure in the hindfoot decreased, and that in the forefoot increased with the prosthesis (Figure 5-B), compared to without the prosthesis (Figure 5-A).
The final follow-up was 7 years after surgery, and no varus or equinus deformity was observed in the patient’s foot. His FIM score was 124 points. The deducted items were 1 point for using a cane while walking and 1 point for using a handrail while using stairs.

Fig. 1. Appearance in the standing position after Chopart amputation. The standing position was stable even without the prosthesis.
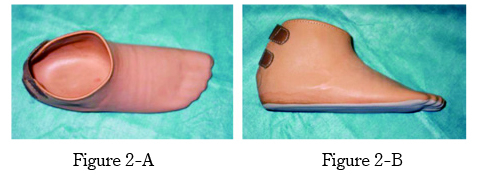
Fig. 2. Foot prosthesis. Figure 2-A:overhead view, Figure 2-B:side view. The foot prosthesis features a belt-type rubber tip and a 10 mm-thick sole, which is designed to attach the rubber tip to the foot. Due to the absence of equinus deformity, the posterior heel and anterior part of the amputation edge have the same height.
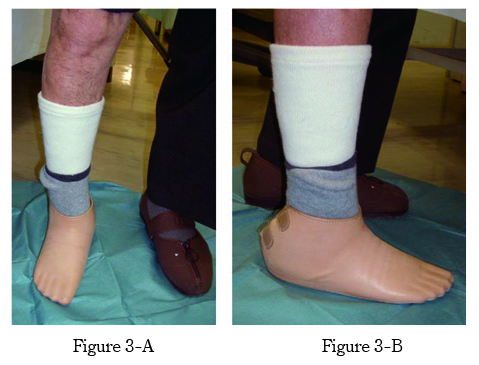
Fig. 3. Standing with a foot prosthesis attached to the right foot. The standing position was stable. Figure 3-A:anterior view, Figure 3-B:side view.
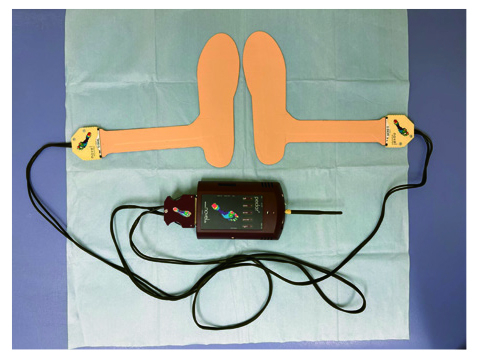
Fig. 4. The plantar pressure while walking was measured using an insole-type pressure distribution sensor (Pedar-X;Novel gmbh, Germany). This device has 99 segmental sensors placed in the insole.
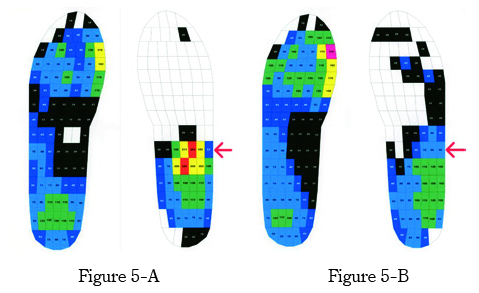
Fig. 5. Plantar pressure while walking without a prosthesis, Figure 5-A. The right foot is the Chopart amputated foot. The numbers in squares indicate the mean maximum pressure at each site. They are displayed in the order of red, yellow, green, light blue, blue, and black, in descending order of pressure. White indicates areas that could not be measured. The pressure at the amputation site was the average of seven sites in the most distal row (sixth row counting from the rear, the row indicated by the red arrows) where the measured values were obtained. There was high pressure on the amputation stump of the right foot.
Plantar pressure while walking with a foot prosthesis, Figure 5-B. The pressure applied to the amputation stump of the right foot is distributed and reduced.
Discussion
Chopart amputation has the advantage of resulting in the affected limb being able to bear weight without a prosthesis4-6) because the heel can be preserved,7,8) which is not the case with lower leg amputation. However, after surgery, the plantar flexor muscles become dominant because of the removal of all the dorsiflexor muscles, and there is a high risk of equinus deformity9,10). To prevent postoperative deformation, in the present case we performed tendon transfer of the tibialis anterior tendon and peroneus brevis tendon, as well as lengthening of the Achilles tendon, to balance plantar-dorsiflexor muscle strength.
Prostheses after Chopart amputation are difficult to fit due to the short remaining tarsal bones11,12). Therefore, it is usually necessary for the patient to wear an ankle-foot-orthosis or a boot-type prosthesis. However, if there is no varus or equinus deformity, the ankle joint has muscle strength, and the foot has stability and support, smooth walking ability can be acquired with the use of a foot prosthesis. Advantages of the foot prosthesis are that it is easy to put on and take off and that it is possible to push off the ground while walking. Disadvantages include difficulty standing and walking stably in patients with weak ankle muscles.
In Chopart’s amputation, the midfoot and forefoot are resected, and the residual tarsal bone is short, making it impossible to push off the ground while walking. As a result, the patient has a limp gait, resulting in a slow walking speed. By wearing the foot prosthesis, it becomes possible to push off the ground while walking, and the walking speed increases. In the present case, the patient’s walking speed was 0.6 m/s without the foot prosthesis but increased by 33% to 0.8 m/s when the patient used the foot prosthesis. He was able to achieve a walking speed almost equivalent to an average 80-year-old (0.9 m/s)13). We believe that the reason for the increase in walking speed is that the prosthesis made it easier for the patient to push off the ground, increasing stride length.
The plantar pressure while walking before the patient started using the prosthesis was high at the amputation stump because the remaining tarsal bones were short in the Chopart amputation. Therefore, there was a risk of forming calluses and ulcers on the amputated stump. When wearing the foot prosthesis, the plantar pressure was decreased by 59%. Before wearing the prosthesis, the pressure was concentrated on the amputated end, but after wearing the prosthesis, the pressure on the amputated end decreased. This finding indicates that the foot prosthesis was able to disperse and reduce the pressure applied to the amputation stump. The increased plantar pressure in the forefoot on the non-amputated side due to wearing the prosthesis may have led to an increase in walking speed.
We investigated walking speed and plantar pressure in a patient following Chopart amputation. Wearing a foot prosthesis improved the patient’s walking speed and decreased plantar pressure at the amputation stump.