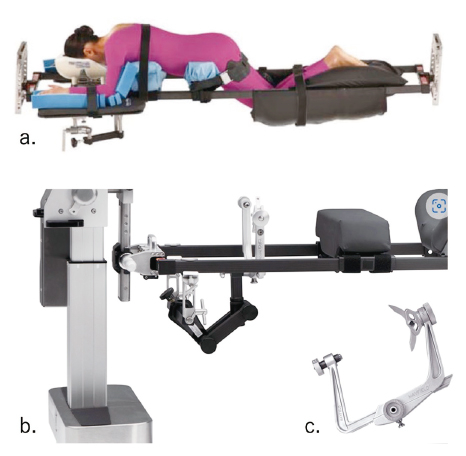
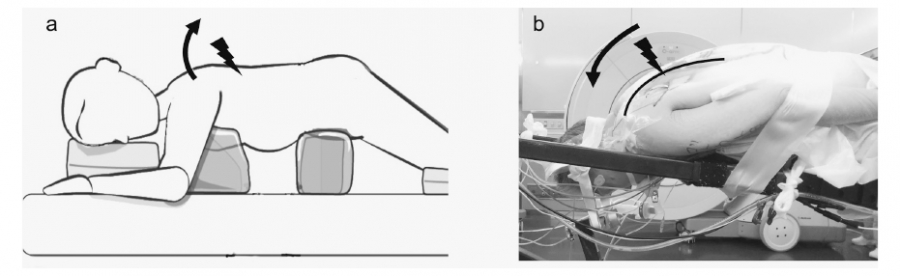
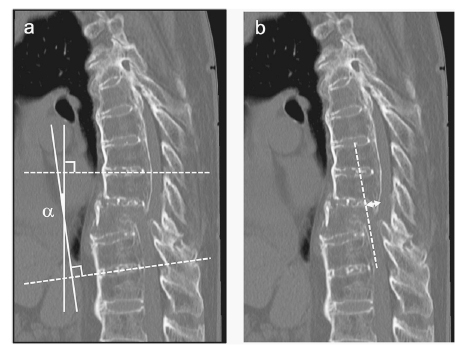
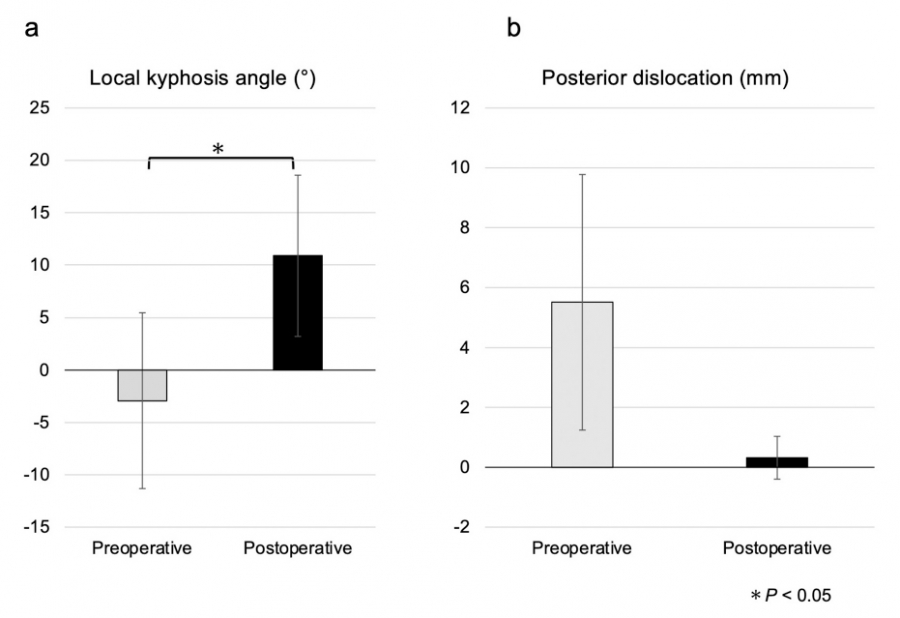
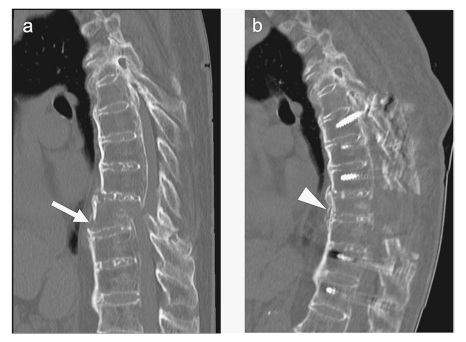
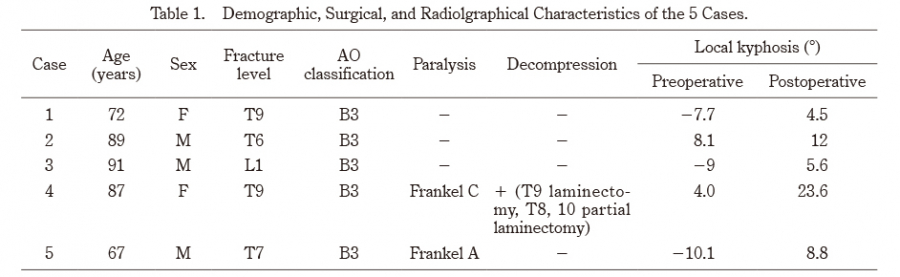
Diffuse idiopathic skeletal hyperostosis (DISH) frequently occurs in the spine, resulting in unstable fractures. Treating thoracolumbar fractures in patients with DISH is often difficult because the anterior opening of the vertebral body is exacerbated by dislocation in the prone position, making reduction difficult. In this study, we introduced a novel skull clamp-assisted positioning (SAP) technique. The patient is placed in a supine position with a skull clamp used in cervical spine surgery before surgery to prevent the progression of dislocation and to restore the patient’s position. Using this method, the mean difference in local kyphosis angle improved from −2.9 (±8.4)° preoperatively to 10.9 (±7.7)° postoperatively. Furthermore, posterior displacement decreased from a preoperative mean of 5.5 (±4.3) mm to 0.3 (±0.7) mm postoperatively. Complications such as neurological sequelae, implant fracture, and surgical site infection were not observed through one year of postoperative follow-up. SAP may decrease invasiveness and complications. Longer-term studies and larger sample sizes are needed to establish long-term efficacy and benefits.
Abstract/References
A reduction method for anterior opening displacement in thoracolumbarvertebral fractures with diffuse idiopathic skeletal hyperostosis using the skull clamp-assisted position
Hiroshi Kobayashi, Kazuyuki Watanabe, Yoshihiro Kobayashi, Kinshi Kato, Takuya Nikaido, Koji Otani, Shoji Yabuki, Shin-ichi Konno, Yoshihiro Matsumoto
-
Hiroshi Kobayashi
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine
-
Kazuyuki Watanabe
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine
-
Yoshihiro Kobayashi
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine
-
Kinshi Kato
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine
-
Takuya Nikaido
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine
-
Koji Otani
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine
-
Shoji Yabuki
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine
-
Shin-ichi Konno
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine
-
Yoshihiro Matsumoto
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine
Abstract
References
1. Resnick D, Niwayama G. Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology, 119:559-568, 1976.
11. Trungu S, Ricciardi L, Forcato S, et al. Percutaneous instrumentation with cement augmentation for traumatic hyperextension thoracic and lumbar fractures in ankylosing spondylitis:A single-institution experience. Neurosurg Focus, 51:E8, 2021.
12. Matsumoto T, Ando M, Sasaki S. Effective treatment of delayed union of a lumbar vertebral fracture with daily administration of teriparatide in a patient with diffuse idiopathic skeletal hyperostosis. Eur Spine J, 24:S573- S576, 2015.
15. Lindtner RA, Kammerlander C, Goetzen M, et al. Fracture reduction by postoperative mobilisation for the treatment of hyperextension injuries of the thoracolumbar spine in patients with ankylosing spinal disorders. Arch Orthop Trauma Surg, 137:531-541, 2017.
16. Ikuma H, Hirose T, Takao S, et al. The impact of the lateral decubitus position in the perioperative period on posterior fixation for thoracolumbar fracture with ankylosing spinal disorder. J Neurosurg Spine, 36:784-791, 2021.
17. Roth C, Ferbert A, Deinsberger W, et al. Does prone positioning increase intracranial pressure? A retrospective analysis of patients with acute brain injury and acute respiratory failure. Neurocrit Care, 21:186-91, 2014.
Figures