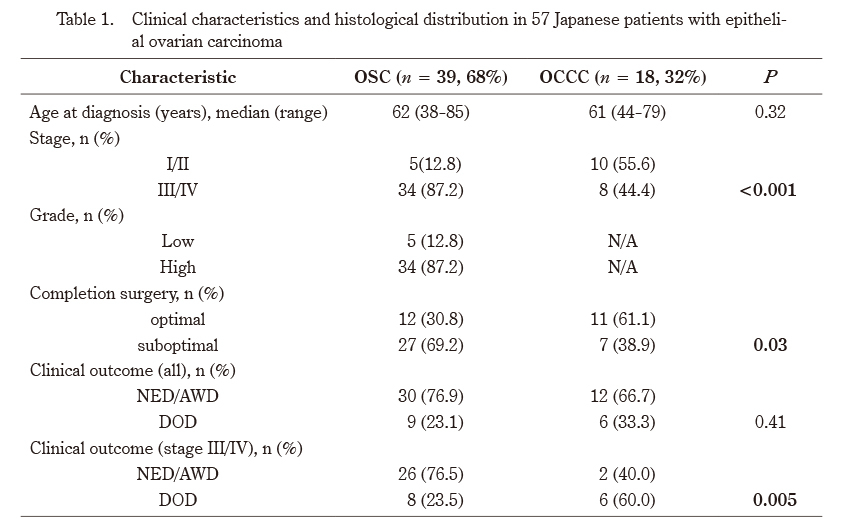
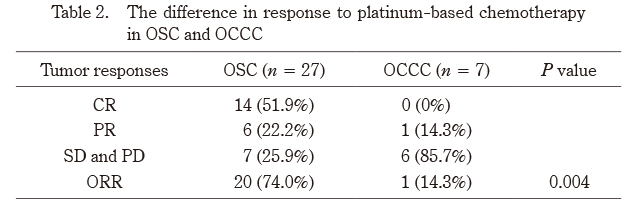
In the current study, we confirmed clinical differences between OSC and OCCC. OCCC tends to be diagnosed earlier than OSC;the rates of OSC and OCC diagnosed at stage I or II were 57–81% and 19-22%, respectively13,14). In general, HGOSC is an aggressive tumor that grows quickly and has often spread throughout the abdominal cavity by the time of diagnosis. Our results indicate that the OSC patients were at a significantly later stage and had a lower rate of completion surgery than the OCCC patients (Table 1). The clinical outcomes of OSC and OCCC significantly differed only in stage III/IV cases, but not in all cases (Table 1). In addition, platinum-based chemotherapy for patients with suboptimal surgical results was more effective in the OSC patients than in the OCCC patients (Table 2). These results support those of previous studies, which reported that OCCC is characterized by platinum resistance and poor prognosis in advanced stage8).
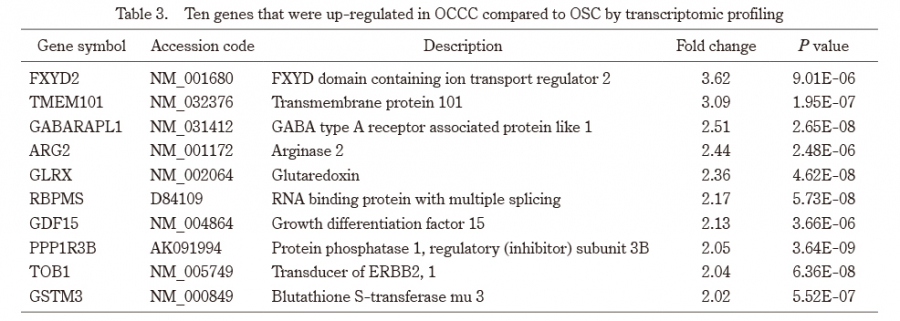
In order to develop a diagnostic tool to differentiate between OCCC and OSC, we identified 10 genes obtained by differentially expressed gene analysis using DNA microarray technology. There have been several reports of comprehensive gene expression analysis for OCCC using cDNA microarrays15–17). The FXYD2, RBPMS, GLRX and TOB1 genes were common in the 10 genes we detected.
The FXYD2 gene encodes the γ-subunit of the Na+/K+-ATPase, which facilitates the egress of sodium, ingress of potassium, and maintenance of the transmembrane potential. Recently, it has been reported that FXYD2 overexpression in OCCC may serve as a promising prognostic biomarker, and can be a therapeutic target for cardiac glycosides that inhibit the Na+/K+-ATPase18). RBPMS protein is a member of a family of proteins that bind to the nascent RNA transcripts, and identify a selective marker of retinal ganglion cells19). GLRX protein acts as a glutathione (GSH)-dependent hydrogen donor for ribonucleotide reductase, and plays a role in the maintenance of cellular thiol redox homeostasis20). Hepatocyte nuclear factors are a subfamily of transcription factors that play multiple roles in the transcription of liver-specific genes21). Among these hepatocyte nuclear factors, HNF1β protein regulates expression of multiple genes implicated in cell differentiation, susceptibility to apoptosis, and glucose metabolism, and is associated with carcinogenesis of various tumors22). In EOC, the overexpression of HNF1β is specific for OCCC, and the incidence of HNF1β immunoreactivity has been reported to differ significantly between OCCC and other histologies23). Since FXYD2, RBPMS, and GLRX are associated with downstream targets of the HNF1β pathway, these genes may play an important role in differential diagnosis or carcinogenesis in OCCC21).
The TOB1 (ErbB-2,1) gene encodes a member of the erbB-2/B-cell translocation gene protein family of anti-proliferative factors that have the potential to regulate cell growth and differentiation. Although decreased expression of TOB1 was reported in various cancers, mostly thyroid, lung, and breast, there have been few reports of down-regulated TOB1 expression in EOC24). Results of the present study indicate that decreased TOB1 expression in OSC compared to OCCC may be associated with clinical features in OSC patients, such as aggressive behavior and advanced stage.
The six genes GSTM3, GABARAPL1, ARG2, PPP1R3B, TMEM101 and GDF15 have not previously been reported to be associated with cDNA microarray in EOC15-17). The GSTM3 gene has traditionally been considered to play a role in the detoxification of electrophiles by GSH conjugation25). Some studies have demonstrated that overexpression of GSTM3 was associated with resistance to cisplatin using a cell line model26). The GABARAPL1 protein is known as one of the homologs in the ATG8 protein, which plays a key role in autophagy processes, acts as a tumor suppressor, and inhibits Wnt signaling through promoting Dvl2 degradation27). UCA1 has been reported to be involved in cisplatin resistance mechanisms in ovarian cancer and bladder cancer, and one of the downregulated mRNAs was GABARAPL128-30). The overexpression of GSTM3 and GABARAPL1 may reflect features of OCCC, such as platinum resistance and poor prognosis. Since there have been few reports on the associations of ARG2, PPP1R3B, TMEM101 and GDF15 with cancer or chemoresistance, we believe that it is important to accumulate more information on these genes in the future.
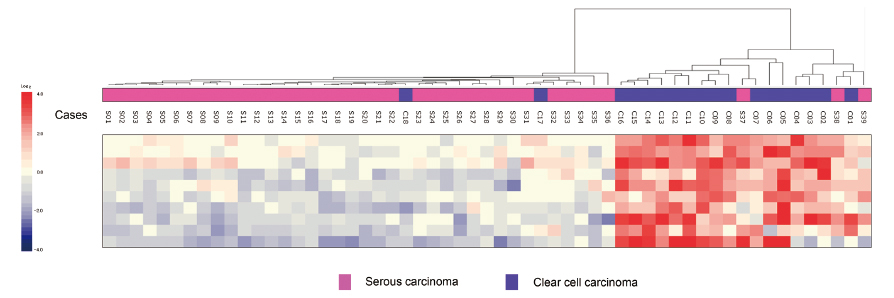
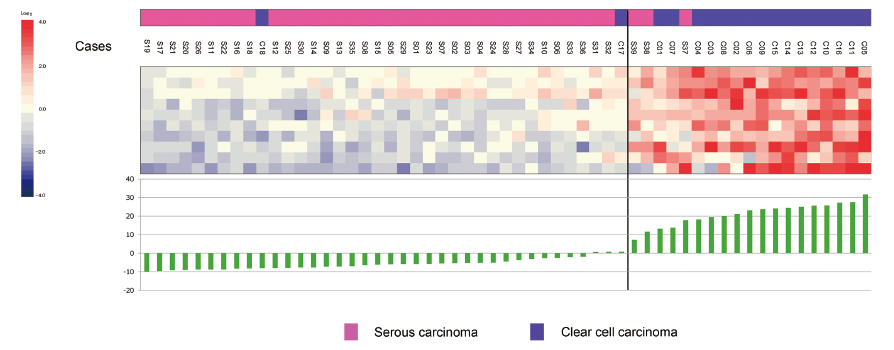
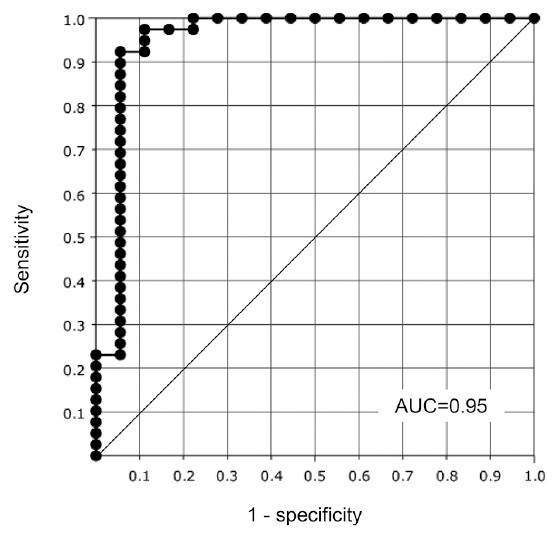
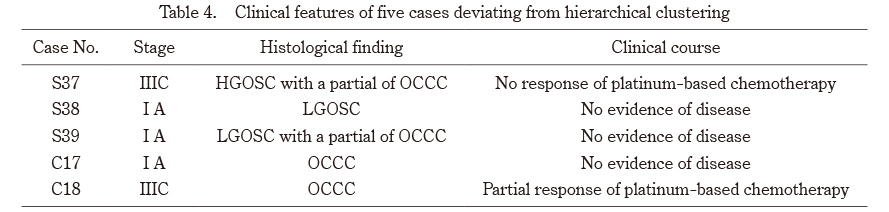
The 57 samples in our study were divided into OSC (n = 39) and OCCC (n = 18) by hierarchical clustering using a gene set consisting of a 10-gene signature (Fig. 1). Three (7.7%) of the 39 OSC cases and two (11.1%) of the 18 OCCC cases were excluded from the clustering. These five cases that were outliers of the clustering tended to be distributed around the cutoff value of the gene expression scoring system (Fig. 2). We performed a clinicopathological evaluation of the five cases that fell outside the clustering. Tumors S37, S38, and S39, which were in the OCCC cluster, showed LGOSC in two cases (S38 and S39) and a partial OCCC component in two cases (S37 and S39) (Table 4). Recently, a dualistic model has been proposed to divide EOC into two broad categories, called type I and type II. Type I ovarian tumors, which arise in a stepwise process from borderline neoplasms, include endometrioid, clear cell, mucinous, and transitional cell carcinomas, as well as LGOSC, while type II tumors, which develop de novo from the tubal and/or ovarian surface epithelium, comprise high grade serous carcinomas, undifferentiated carcinomas, and carcinosarcomas. Since cases S38 and S39 in the present study were pathologically LGOSC, their gene expression is expected to resemble OCCC included in type I more than HGOSC included in type II, considering their molecular biological classification. Although HGOSC is usually sensitive to platinum-based chemotherapy compared to OCCC, tumor S37 had no response. In our study, the ORRs in stage III/IV OSC and OCCC patients with suboptimal surgical results were 74% and 14%, respectively (Table 2). Tumor S37, grouped as OCCC by hierarchical clustering, had the OCCC characteristic of chemotherapy resistance. Tumor C18, grouped as OSC, also had the OSC characteristic of chemotherapy sensitivity. In the present study, we constructed a gene expression scoring system for distinguishing OSC from OCCC using 10 selected genes (Fig. 2). Introduction of the scoring system would make it easier to differentiate OSC from OCCC. Since there have been few studies in which a gene expression scoring system was constructed for use when diagnosing cancer, this scoring system would be a novel and powerful diagnostic tool12).
There are several limitations to this study. First, the main limitations of our study were its retrospective design and relatively small sample size. Second, there was no independent cohort to validate the proposed biomarkers. Third, EOC is histologically heterogeneous, including not only OSC and OCCC but also endometrioid carcinoma and mucinous carcinoma. Furthermore, OSC is histologically classified as LGOSC and HGOSC, each with different clinical and molecular features. Since the frequency of mixed-type histology has been reported to be 6% of all EOC cases, the identification of a gene signature for five major pathological EOC subtypes may be necessary for better differential diagnosis31).
In conclusion, OSC and OCCC are two major histological types of EOC, with distinctly different biological features and clinical behaviors. The results of our study suggest that the 10 candidate genes selected using DNA microarray technology would serve well to distinguish OSC from OCCC. Furthermore, the systemic identification of a differentially expressed 10-gene signature may shed light on variances in carcinogenesis and provide a theoretical basis for OCCC’s resistance to chemotherapy.