In the present study, we measured testicular stiffness using ultrasound strain elastography to examine whether we can estimate testicular development and histopathological changes after orchiopexy, and discuss the optimal timing of orchiopexy.
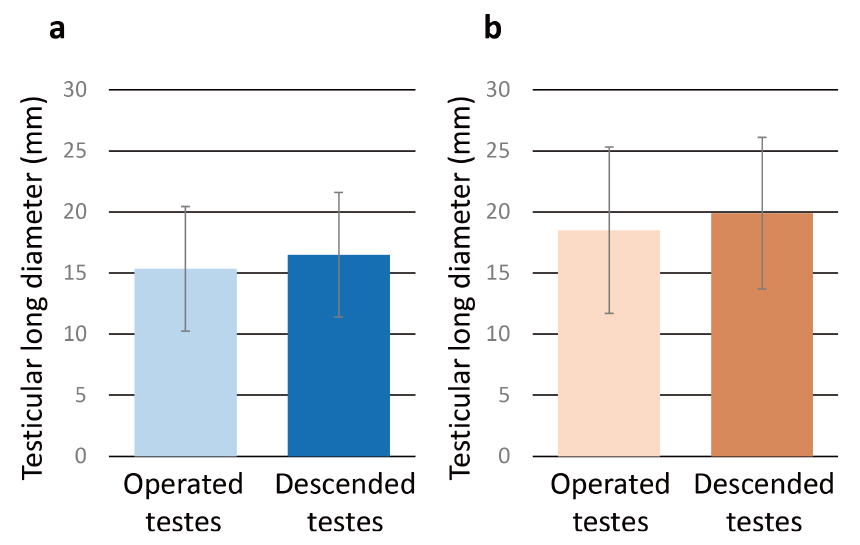
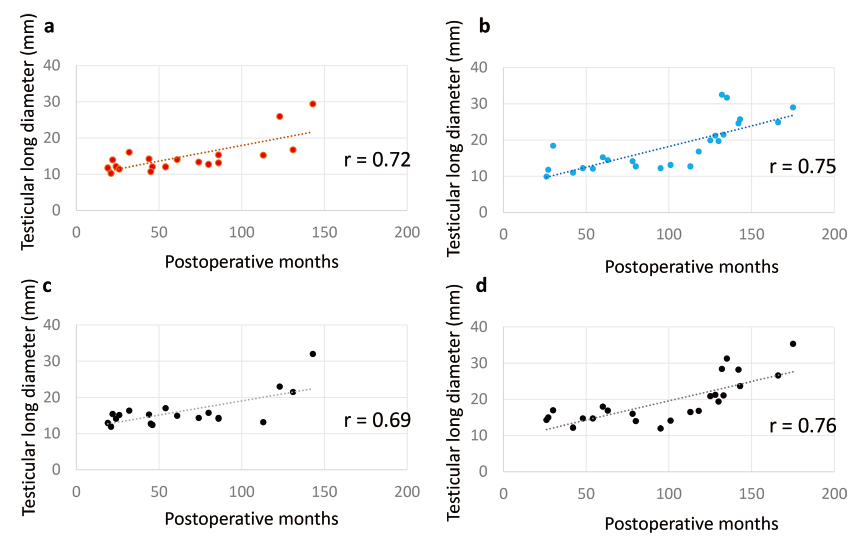
Significant histopathological changes in some patients with undescended testis have been observed, which led to disturbances of spermatogenesis and male infertility in the future9). Several studies demonstrated testicular fibrosis in adults with a history of cryptorchidism10). There are a limited number of tools available to evaluate these histopathologic changes in testes after orchiopexy. Although testicular biopsy can be used to assess histopathological changes such as fibrosis, it is not recommended in the follow-up period because of its invasiveness. Measurement of testicular volume and size by ultrasonography is a noninvasive method to evaluate testicular development. In the present study, a significant positive correlation between the testicular long diameter of both operated testis and postoperative months was found regardless of the timing of orchiopexy. However, testicular volume and size may not always reflect testicular histopathological change. Therefore, a non-invasive procedure to estimate testicular histopathological change is needed.
Ultrasound elastography is a relatively modern evolutionary technique of sonographic imaging. Originally, it was developed to assess tissue stiffness with the potential of differentiating between benign and malignant tumors11). Complementary to conventional ultrasonography, elastography can be used to assess quantitative and qualitative information about tissue stiffness12) and estimate the degree of fibrosis as a result of tissue damage in various organs, including the liver, kidney, and thyroid11,13-16). Therefore, elastography is expected to be used to predict pathological status without tissue biopsy. In the present study, we measured the testicular stiffness of undescended testes after orchiopexy using ultrasound strain elastography.
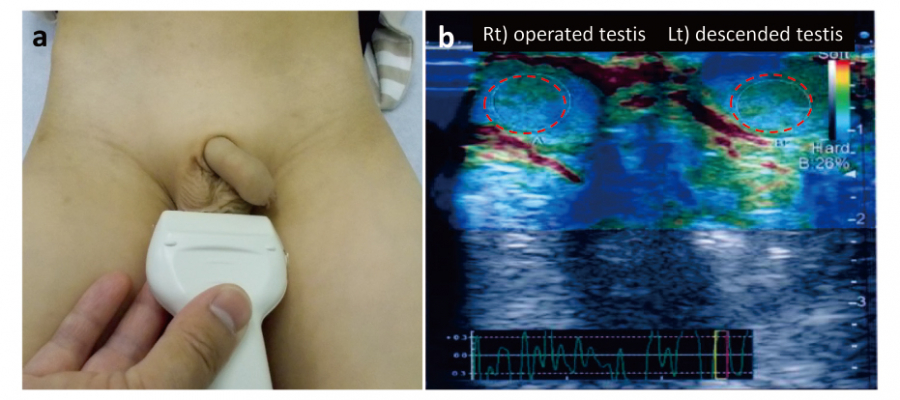
There are two main methods of measuring stiffness in ultrasound systems:shear wave elastography (also known as transient elastography; SWE), which is a quantitative evaluation using the propagation velocity of shear waves, and strain elastography (also known as static or compression elastography), which is a relative evaluation that visualizes differences in tissue distortion7). Some reports have evaluated testicular stiffness in patients with undescended testes8,17-22), most of which utilized SWE. However, SWE does not take into account individual differences in testicular stiffness because it is used for quantitative evaluations of individual testes. In the present study, therefore, we used strain elastography to evaluate testicular stiffness. Previous reports of testicular stiffness by strain elastography showed that the strain ratios were measured as the ratios of the elasticities of subcutaneous fat tissue to the elasticities of the undescended testes8). In the present study, we measured the strain ratios as the ratios of the elasticities of contralateral descended testes to the elasticities of the operated testes, because they can be visualized in the same field of view by strain elastography simultaneously, and the relative testicular stiffness can be evaluated by causing bilateral testicular tissue distortion with an echo probe. We considered that strain elastography could directly compare the difference in testicular stiffness between the operated testis and the contralateral descended testis, reduce individual differences, and make a more accurate evaluation of postoperative changes occurring in the operated testis.
There are some reports that have investigated the testicular stiffness of undescended testes using SWE17-21). Shin et al. evaluated the differences and changes in testicular volume and elasticity in the normal and undescended testes of children using SWE and reported that instead of increasing volume and decreasing stiffness of normal testes during development in the first 60 months of age, undescended testes had smaller volume and increased stiffness when compared to normal testes. The contralateral descended testes of patients with unilateral undescended testes showed increased volume without stiffness change17).
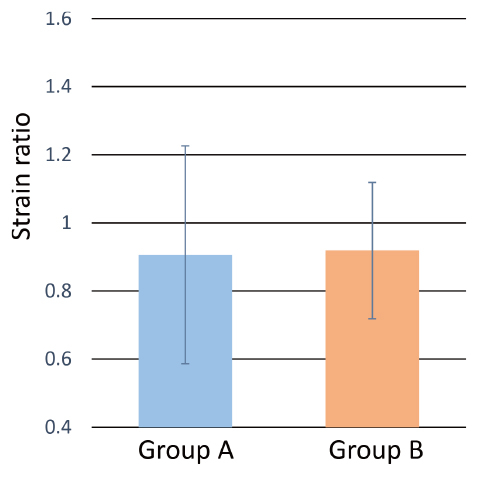
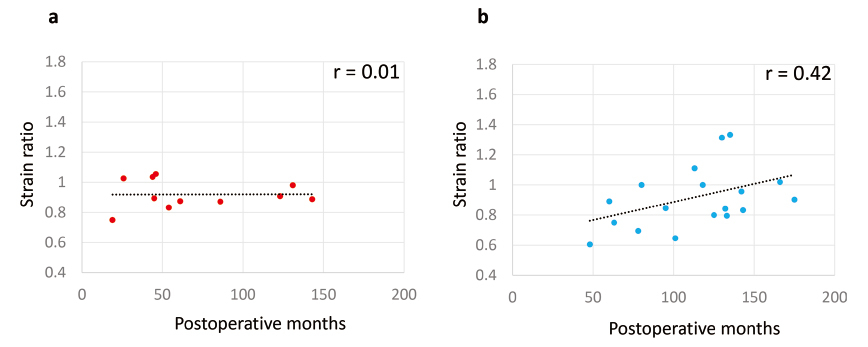
In the present study, the mean strain ratios were 0.90 ± 0.32 and 0.92 ± 0.20 in the patients who received orchiopexy at age < 2 years and ≥ 2 years, respectively, suggesting that testicular stiffness was similar between the operated and contralateral descended testes. However, the strain ratio remained constant with postoperative months in the patients who received orchiopexy at age ≤ 2 years, while it tended to increase with postoperative months in boys who had received orchiopexy at age ≥ 2 years, although a significant change was not found. Interestingly, variations in the strain ratios were observed in patients who had received orchiopexy at age ≥ 2 years. Some patients had a high strain ratio, while others did not, indicating that the testicular stiffness of the operated testis differed from patient to patient. The variation may be due to a mix of cases that were missed by screening despite having clear undescended testes, or mild cases that were not determined to have undescended testes by screening. Patients with a history of undescended testis do not always experience disturbances of spermatogenesis. Some patients might experience testicular damage and male infertility, while others are able to preserve spermatogenesis and fertility. Therefore, strain elastography may help to distinguish between these types of patients. Two previous reports showed testicular stiffness of undescended testes after orchiopexy. Hattapoğlu et al. demonstrated that the median SWE values of testes were significantly higher in operated undescended testes than in descended and normal testes18). Durmaz et al. also demonstrated that the testicular stiffness of operated testes was significantly higher than those of the contralateral descended testes and undescended testes20). Since undescended testes have reduced numbers and delayed maturation of germ cells, they can induce interstitial fibrosis and, consequently, higher testicular stiffness20). Evaluation of testicular stiffness may be useful to estimate testicular histopathological changes such as interstitial fibrosis and the severity of histologic damage in each patient with unilateral undescended testes who undergoes orchiopexy, although further study is needed to confirm this.
The optimal age for orchiopexy remains a controversial issue, although many recent findings suggest that early intervention may be beneficial. We demonstrated in this study that the strain ratio tended to increase with postoperative months in the patients who received orchiopexy at age ≥ 2 years, while it remained constant with postoperative months in the patients who had received orchiopexy at age < 2 years. Our data may support those of previous reports, which recommended orchiopexy as early as possible to avoid testicular damage.
There are some limitations to the present study. First, the sample size was relatively small and future studies will require larger study populations. Second, we did not show a statistically significant correlation between the strain ratio and post-operated months. Third, we also did not investigate a correlation between the testicular stiffness and testicular histopathological findings. Since testicular biopsy is no longer indicated for undescended testes, we cannot obtain histopathological data from the patients. Forth, one operator performed all of the examinations, and we did not evaluate interobserver variability. Although Agladioglu et al. have shown that the interobserver agreement of ultrasound strain elastography was excellent for the elasticity pattern and the concordance of the strain ratios between the observers was excellent22), this should be further explored in future studies. Fifth, we did not measure pre-operative stiffness, and therefore, could not compare the stiffness between pre- and post-operated testis. This is due to the measurement method of testicular stiffness by ultrasound strain elastography. As described above, we measured the strain ratios as the ratios of the elasticities of contralateral descended testes to the elasticities of the operated testes. The testicular stiffness was evaluated by causing bilateral testicular tissue distortion with an echo probe. This method is characterized by that both testes must be visualized in the same field of view by strain elastography simultaneously. Therefore, we cannot measure the stiffness of pre-operated testis since pre-operative undescended (inguinal) testis and descended (scrotal) testis cannot be visualized in the same field of view in the ultrasound image because of the distance between both testes. Because this is a preliminary study, further study will be needed.