We here present a case of cerebral infarction, likely due to hypotension induced by 5-ALA, exacerbated by antihypertensive and antianginal agents.
5-ALA-induced hypotension is not a rare phenomenon. Therefore, extra factors combined with 5-ALA-induced hypotension likely contributed to development of cerebral infarction in our patient.
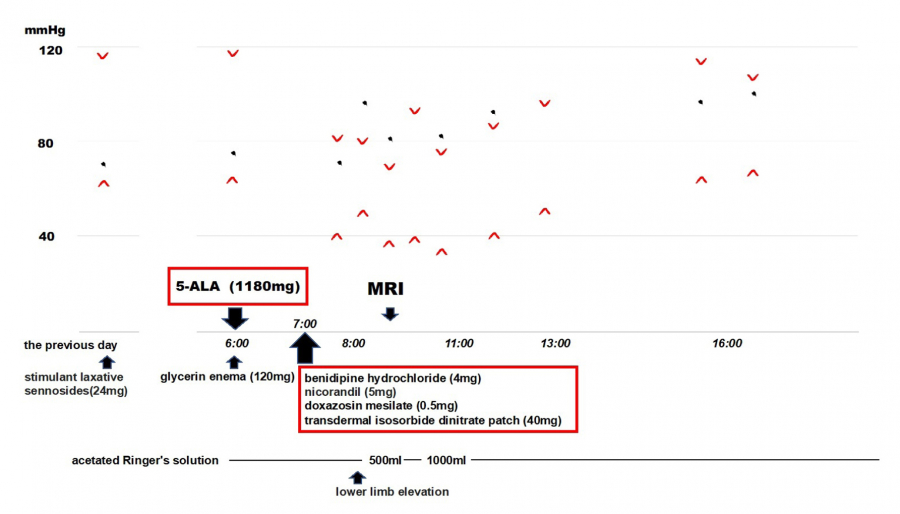
The mechanism by which 5-ALA induces hypotension is not clearly understood; however, nitric oxide released from vascular endothelial cells may be involved in vessel dilation, which in turn depresses blood pressure5). Also, nicorandil and isosorbide dinitrate are vasodilators that acts as nitric oxide donors6). Nitric oxide has a vasodilatory effect that could accelerate 5-ALA induced hypotension. Ivan et al. reported that antihypertensive drugs could be a risk factor in 5-ALA-induced hypotension7). Our patient took a calcium antagonist, alpha-blocker, nicorandil, and also applied a transdermal isosorbide dinitrate patch an hour after 5-ALA administration. These drugs, which have vasodilatory effects, could have exacerbated the subsequent hypotension. Since we did not measure blood pressure in short intervals after administration of 5-ALA, the patient may have been taking antihypertensive and antianginal agents even after his blood pressure began to drop. In most case, antihypertensive drugs like calcium channel blocker and α1-adrenergic receptor antagonist are continued during perioperative periods8). Generally, antianginal agents that act as nitric oxide donors, which in our case were nicorandil and a transdermal isosorbide dinitrate patch, were administered throughout the perioperative period9). If we had been aware of this patient’s high risk of hypotension, we might have withheld them and, if necessary, administered them intravenously during surgery.
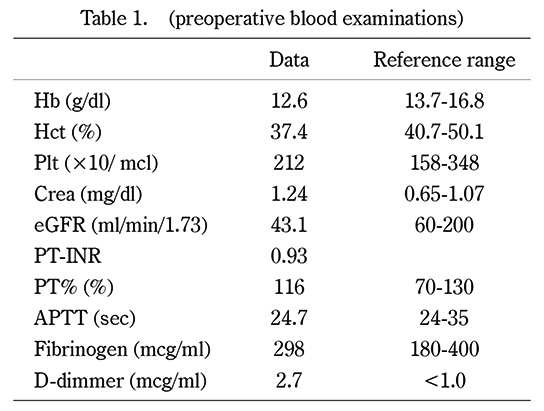
Although our patient had not been diagnosed with renal failure, renal dysfunction was observed prior to the operation. Miyakawa et al. reported that age >80 years, BMI >25, and estimated glomerular filtration rage (eGFR) <45 are significant risk factors for the development of severe hypotension after oral ALA administration10). Thus, our patient was at high risk for developing hypotension with oral administration of 5-ALA.
Additionally, our patient was scheduled to undergo both PDD-TUR-BT and right radical nephroureterectomy. This required preoperative abdominal preparation, which is not usually done for PDD-TUR-BT alone. Although the patient was hydrated from the time of admission, the stimulant laxative and glycerin enema may have contributed to dehydration, which, in turn, could have led to the development of hypotension.
We managed the hypotension by passive leg raising procedure and fluid therapy only. Retrospectively, we should have considered administering vasoactive agents immediately to facilitate the normalization of cerebral perfusion.
The time of onset of our patient’s cerebral infarction was unclear. That it was a wake-up stroke was unlikely because he did not report any abnormalities before 5-ALA administration. We speculated that the cerebral infarction occurred while the patient remained quietly in bed, covered by a blanket to shield him from the light, after 5-ALA administration.
Generally, a DWI–FLAIR mismatch, which means cerebral infarction, occurs within 3 or fewer hours after an ischemic event11). In our case, both DWI and FLAIR images exhibited high signals, indicating that a cerebral ischemic event may have occurred 3 or more hours prior to the scan. This would mean that his cerebral ischemic event had already occurred before the hypotension was first noted and confirmed on a bed-side monitor. Since the patient’s blood pressure wasn’t closely monitored after administering 5-ALA at that time, it is difficult to determine exactly when the hypotension occurred.
Prior to this case, we had experienced several cases of 5-ALA-induced hypotension that was recognized in the operating room; in one case, surgery was aborted. In other cases, surgery was managed by maintaining anesthesia while using vasopressors and catecholamines. The occurrence of ischemic attack symptoms fortuitously allows preoperative awareness. If the anesthesia had proceeded without symptoms, further severe hypotension could have occurred due to anesthesia, possibly resulting in significant stroke sequelae. Had the hypotension been detected prior to taking the usual antihypertensive or antianginal agents, they could have been discontinued. Therefore, we conclude that patients at high risk of developing hypotension after 5-ALA administration would be better observed where blood pressure could be monitored regularly.
We were unable to determine the mechanisms of our patient’s cerebral infarction. The infarction was only in the cortex area, suggesting that it was embolic. Even though the preoperative D-dimer was elevated, deep vein thrombosis of the lower extremities and intracardiac thrombus were not detected during preoperative examination. And also, we did not detect atherosclerotic stenosis nor thrombosis by either carotid artery ultrasound or magnetic resonance imaging.
D-dimmer could be elevated even in the absence of thrombosis because most cancers are associated with hypercoagulable state12). In this condition, thrombosis could have been formed after hypoperfusion with 5-ALA-induced hypotension.
Since the patients took antihypertensive and antianginal agents after administration of 5-ALA, in both these contributed to the sustained hypotension in our case. The relationship between 5-ALA-induced hypotension and the cause of cerebral infarction is not clear because 5-ALA-induced hypotension is not rare. Therefore, it is likely that the hypotension caused by 5-ALA was accelerated by the antihypertensive and antianginal agents, and the dehydration caused by laxatives and enemas might contribute to the hypotension, resulting in development of his cerebral infarction