

Isolated fallopian tube torsion (IFTT) is defined as torsion of only the fallopian tube without any ovarian involvement1). Although IFTT was considered to be rarely responsible for gynecological acute abdomen, its actual incidence was unknown and may be higher than that reported in the previous literature1,2). In this article, we present 4 cases of IFTT that were diagnosed and successfully treated by laparoscopic surgery.
The content of research paper
Four cases of isolated fallopian tube torsion successfully treated with laparoscopic surgery:A case series.
Riho Yazawa, Hiroyuki Yazawa, Kazuki Anjyo, Akari Inazuki
Author information
-
Riho Yazawa
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
-
Hiroyuki Yazawa
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
-
Kazuki Anjyo
Junior Resident, Fukushima Red Cross Hospital
-
Akari Inazuki
Junior Resident, Fukushima Red Cross Hospital
Introduction
Cases
The detailed characteristics of Cases 1-4 are presented in Table 1.
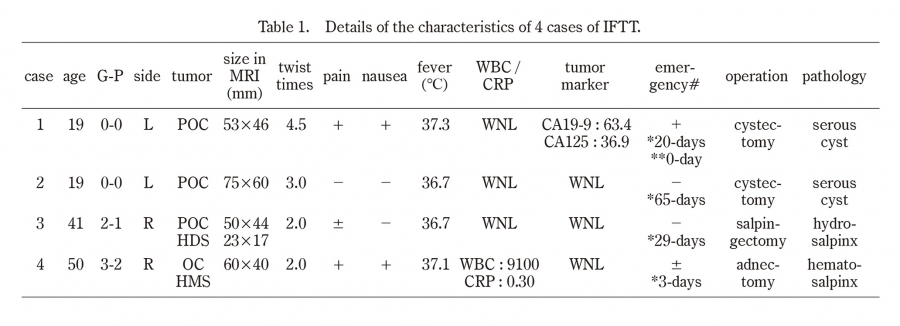
Table 1.
Details of the characteristics of 4 cases of IFTT.
IFTT:isolated fallopian tube torsion, POC :paraovarian cyst, HDS :hydrosalpinx, HMS :hematosalpinx, OC:ovarian cyst
WNL: within normal limits. G-P: gravida and para.
#emergency: +: emergency surgery, -: scheduled surgery, ±: sub emergency surgery
*days from initial consultation to surgery, **days from abdominal pain to surgery.
Case 1.
A 19-year-old woman with no history of sexual intercourse and no significant medical history was referred to our department for treatment of bilateral cystic pelvic masses with left abdominal pain. Magnetic resonance imaging (MRI) revealed bilateral cystic masses in the pelvic cavity, showed low signal intensity on T1-weighted images (WI) and high signal intensity on T2-WI, leading to the diagnosis of bilateral paraovarian cysts (POCs) (Fig. 1A, B). The patient’s abdominal pain was mild and resolved spontaneously, and she was followed up as an outpatient at her request. Twenty days later, however, she returned to the hospital with recurrent left lower abdominal pain, and under suspicion of adnexal torsion, emergency laparoscopic surgery was performed on the same day. Laparoscopic findings revealed bilateral POCs with normal-sized bilateral ovaries. The left fallopian tube was twisted 4.5 times, and the POC and fallopian tube showed purple discoloration, leading to a diagnosis of IFTT (Fig. 1C, D). After the torsion was released, the color of the fallopian tubes improved, and enucleation of the POC was performed. POC enucleation was also performed on the right side (Fig. 1E, F). Postoperative histopathology revealed bilateral POCs with no malignant findings. The patient’s postoperative course was good.
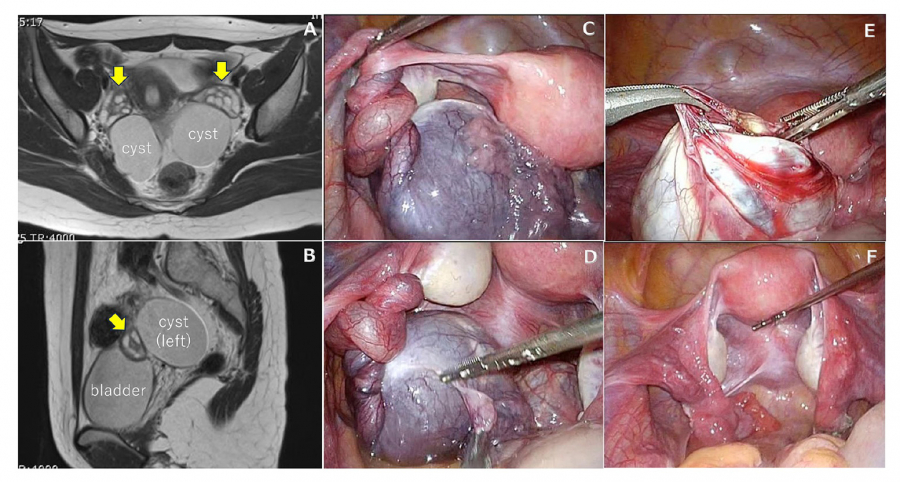
Fig. 1.
MRI and laparoscopic surgical findings in Case 1.
MRI showed bilateral simple cystic tumors in the pelvic cavity (A) and bilateral normal ovaries adjacent to the cystic tumors (A, arrows), leading to the diagnosis of POCs. Laparoscopic findings revealed a left POC and a distal fallopian tube twisted 4.5 times, and IFTT was diagnosed (C, D). The left side of the torsion was released, the bilateral POCs were enucleated, and the surgery was completed (E, F).
Case 2.
A 19-year-old woman with no history of sexual intercourse was referred to our department because of a 7-cm pelvic mass. The patient had no abdominal pain. MRI revealed a 7-cm left cystic mass in the pelvic cavity, with a normal ovary adjacent to the cyst. The cystic mass showed low signal intensity on T1-WI and high signal intensity on T2-WI, leading to a diagnosis of POC (Fig. 2A, B). Laparoscopic surgery was scheduled for about 2 months later. Surgery showed that the left fallopian tube was twisted 3 times, involving a POC, with no color change, and the diagnosis of IFTT was made (Fig. 2C, D). After the torsion was released, enucleation of the POC was performed (Fig. 2E, F). Postoperative histopathology revealed POC with no malignant findings. The patient’s postoperative course was good.
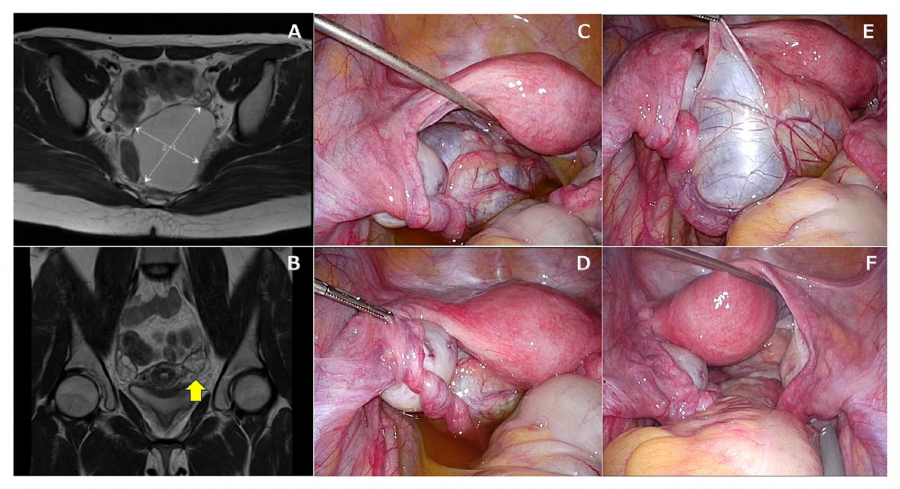
Fig. 2.
MRI and laparoscopic surgical findings in Case 2.
MRI showed a 75 mm × 60 mm simple cystic tumor on the left side of the pelvic cavity (A) and a left normal ovary adjacent to the cystic tumor (B, arrow), leading to the diagnosis of POC. Laparoscopic findings revealed a left POC and a distal fallopian tube twisted 3 times, and IFTT was diagnosed (C, D). After the torsion was released, the POC was enucleated and the surgery was completed (E, F).
Case 3.
A 41-year-old woman, gravida 2, para 1 requested laparoscopic surgery for occasional lower abdominal pain that she had been experiencing since a previously diagnosed right 5-cm hydrosalpinx. MRI revealed a bifid cystic tumor on the right side of the pelvis, with low signal intensity on T1-WI and high signal intensity on T2-WI, as well as a normal ovary adjacent to the tumor (Fig. 3A, B). These findings led to the diagnosis of POC and hydrosalpinx. Laparoscopic surgical findings included a right POC and hydrosalpinx, and the fallopian tube was twisted 2 times, involving the POC, resulting in a diagnosis of IFTT (Fig. 3C, D). Right salpingectomy was performed because the patient had no desire to have a baby (Fig. 3E, F). Postoperative histopathology revealed hydrosalpinx with no malignant findings. The patient’s postoperative course was good.
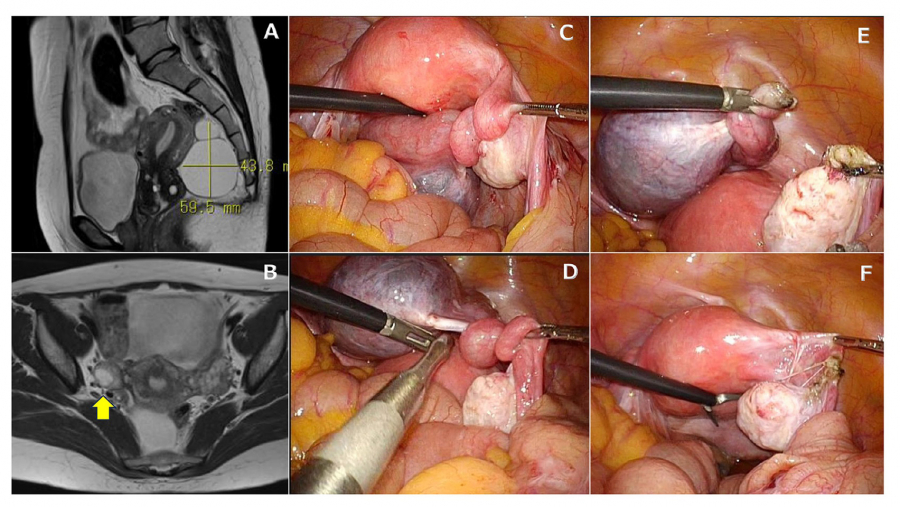
Fig. 3.
MRI and laparoscopic surgical findings in Case 3.
MRI showed a bifid cystic tumor with large and small sections on the right side of the pelvic cavity (the large cyst was a POC, and the small cyst was a hydrosalpinx) (A), and a normal ovary adjacent to the cystic tumor (B, arrow), leading to the diagnosis of POC. Laparoscopic findings revealed a right POC and an enlarged distal fallopian tube twisted 2 times, and IFTT was diagnosed (C). Right salpingectomy was performed, and the surgery was completed (E, F).
Case 4.
A 50-year-old woman, gravida 2, para 1, with right lower abdominal pain was referred to our department on suspicion of adnexal torsion. MRI showed a right hydrosalpinx 3 × 6 cm in size and a right ovarian cyst 3 cm in diameter (Fig. 4A, B). Adnexal torsion was suspected; thus, laparoscopic surgery was performed. The right fallopian tube, including the hydrosalpinx but not the ovary, was twisted 2 times, and a diagnosis of IFTT was made and a right adenectomy was performed (Fig. 4C–F). Postoperative histopathology revealed a luteal cyst in the right ovarian cyst as well as hematosalpinx. The patient’s postoperative course was good.
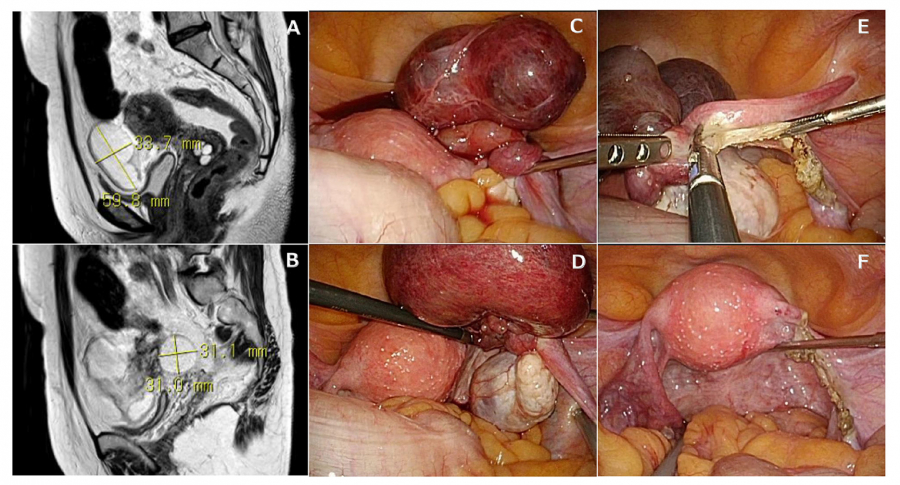
Fig. 4.
MRI and laparoscopic surgical findings in Case 4.
MRI showed a 6 cm × 4 cm cystic tumor anterior to the uterus on the right side of the pelvic cavity (A), and a normal ovary with a small cyst adjacent to the ipsilateral cystic tumor (B), leading to the diagnosis of a right ovarian cyst and hydrosalpinx. Laparoscopic findings revealed that the right fallopian tube, including hydrosalpinx, was twisted 2 times (C), and a small cyst was found in the ovary but without torsion (D); IFTT was diagnosed. Right adenectomy was performed and the surgery was completed (E, F).
Discussion
IFTT is defined by torsion of only the fallopian tube without any ovarian involvement1). The condition was first reported in 1980 by Bland-Sutton3), and its incidence was unknown until recently. IFTT was considered to be one of the rarest causes of gynecological acute abdomen, with a previously reported frequency of 1 in 500,000 to 1.5 million4,5). In a recent study, however, Hagege et al. described encountering 9 cases of IFTT in 3 years, representing 14% of all patients with proven adnexal torsion2). According to previous reports on the frequency of adnexal torsion6,7), the authors estimated the frequency of IFTT to be 1 in 100,000 women per year2), which is more common than previously reported. Consistent with their findings, a review of surgically excised benign ovarian tumors at our hospital over the past 10 years showed that IFTT occurred in 4 of 43 cases of adnexal torsion (9.3%), also suggesting that it is not as rare as previously reported (unpublished data).
The causes of IFTT can be broadly classified into those intrinsic or extrinsic to the fallopian tubes. The former include hydrosalpinx, hematosalpinx, tubal tumor, tubal elongation, and tubal malformation, while the latter include POCs, pelvic infection, laxity of the ligament due to pregnancy, etc.8) In our IFTT, 3 patients had POCs (extrinsic) and 1 had hematosalpinx (intrinsic).
POCs are found in about 3-20% of adnexal tumors9,10), and they develop from the peritoneal mesothelium, paramesonephric remnants, or occasionally from mesonephric remnants11). POCs are generally benign; borderline or even malignant paraovarian tumors are rarely encountered12). In a review of 20 cases of IFTT with POCs, Qian et al. reported that IFTT was more common in young patients, with 13 of the 20 cases occurring in adolescence at a median age of 15 years13). The mean tumor diameter at the time of fallopian tube torsion was 5 cm (2-9 cm), and it is assumed that tumors with a diameter greater than 5 cm are at high risk of torsion13). In our case series, Cases 1-3 had POCs of 5-7 cm in diameter, and the risk of torsion was therefore considered to be high. On the other hand, a study of 30 patients with IFTT who were under 15 years of age reported that the most common cause was hydrosalpinx, in 10 cases14).
It has been reported that IFTT is characterized by diffuse rather than local abdominal pain, and that compared to adnexal torsion, symptoms are often vague and indistinct, which often makes the diagnosis difficult2,11). In our case series, emergency surgery due to pain was performed only in Case 1, while Case 4 was a semi-emergency and in Cases 2 and 3, the diagnosis of ITFF was made incidentally during surgery scheduled for a POC. Thus the percentage of these cases in which emergency surgery was required was significantly lower than the rate of such surgery for adnexal torsion at our hospital (67%, 26 of 39 cases, unpublished data). In contrast to adnexal torsion, IFTT does not involve large ovarian arteriovenous vessels; thus, the degree of blood flow disturbance is assumed to be less severe. This may be due in part to mild symptoms caused by congestion and ischemia.
The diagnosis of IFTT appears to be relatively difficult. Although the “break sign” and “tapered sign,” which indicate tapered cyst structures, and the “coiling sign,” which reflects coiled fallopian tubes, are considered to be characteristic features of IFTT15), it is often difficult to make a preoperative diagnosis based on these findings. In a report, only 8 of 27 cases of IFTT were diagnosed preoperatively by ultrasound16). Even in our series, we suspected IFTT in 2 of the 4 cases (Cases 1 and 4), where the diagnosis of POC and hydrosalpinx was possible by preoperative imaging.
Surgical treatment for IFTT includes fallopian tube preservation surgery (detorsion ± cystectomy) and fallopian tube resection (salpingectomy). Even if the fallopian tubes are ischemic due to torsion, they can be preserved if blood flow can be resumed early by detorsion. Of the 4 cases of IFTT described here, salpingectomy and adenectomy were selected for Cases 3 and 4, in which there was no desire to preserve fertility, while tubal preservation surgery with detorsion and paraovarian cystectomy was chosen in Cases 1 and 2 because the patients were younger and it was judged that the fallopian tubes could be preserved with detorsion.
In adnexal torsion, it has been reported that a delay in surgery of more than 10 hours increases the frequency of necrosis17). In IFTT, it was reported that adnexal necrosis progressed when pain persisted for more than 24 hours, leading to salpingectomy being selected more often in such cases18). Qian L et al. reported that salpingectomy was performed more frequently in cases with vomiting, suggesting that not only the duration of pain but also its degree is an important factor in the degree of necrosis13). These authors also found that there was no association between the number of torsion rotations and the degree of necrosis13). In our Case 1, the fallopian tubes were twisted 4.5 times, but after the torsion was released, the color tone recovered, and the fallopian tubes could be preserved without necrosis. This case reminded us of the importance of accurate diagnosis and early intervention, especially in patients in the age group where tubal preservation is desirable.
Conclusion
Although IFTT was previously considered to be very rare, recent reports and the data at our hospital suggest that its incidence may have been underestimated, as it accounts for approximately 10% of adnexal torsion cases, including those that are asymptomatic. Since most patients who develop IFTT are young, surgical intervention to preserve the fallopian tubes should be chosen as early as possible, if IFTT is suspected from the clinical course and the imaging modalities such as MRI. Gynecologists need to be aware of this disease, to understand its pathogenesis, and to be able to diagnose it as early as possible.
Conflicts of interest
The authors have no conflicts of interest to declare.
Patient consent
We obtained informed consent from all patients for the publication of this work.