In the field of trauma, compared with resuscitative thoracotomy, REBOA is a relatively less invasive intervention for life-threatening hemorrhage. Recently, REBOA has also emerged as a novel procedure for preventing significant obstetric hemorrhage13). REBOA involves the insertion of a balloon catheter device that can be placed at the bedside. Conventionally, REBOA is most frequently used in trauma, but there is growing evidence supporting its use in non-traumatic hemorrhagic events, including gastrointestinal bleeding, ruptured viscera, aneurysms, and obstetric bleeding18). The first report on the use of REBOA in the field of obstetrics was in 1995, in a case of PAS19). Since then, over 1,000 cases of aortic balloon occlusion have been reported in obstetrics, mainly for cases with PAS to control obstetric hemorrhage during cesarean hysterectomy20).
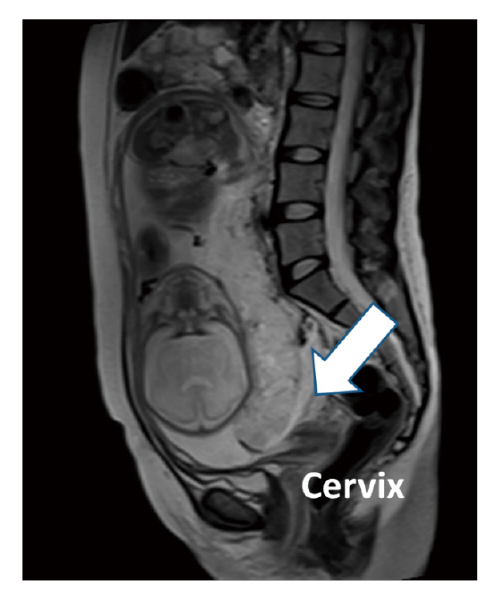
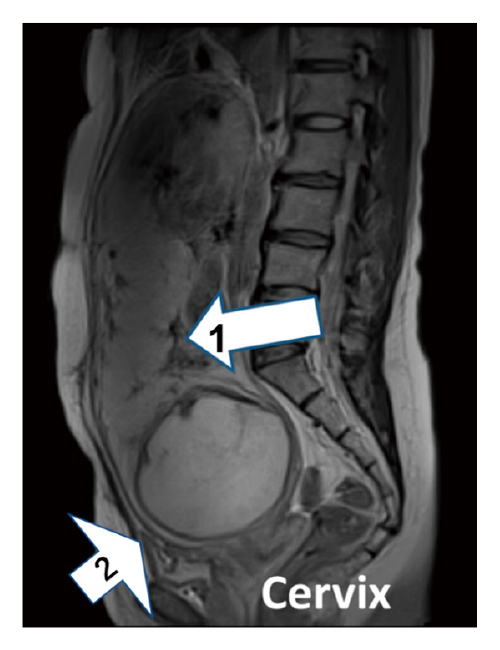
In addition to the typical PAS characterized by placenta previa and previous cesarean section history, the concept of unexpected PAS, which is defined as the occurrence of severe obstetric hemorrhage for the first time at the time of delivery, is growing4,6-8). Unexpected PAS is usually defined as unsuspected PAS at the time of delivery due to the absence of placenta previa, which is the typical form of conventional PAS4,6-8). Of note, unexpected PAS is an important concern because it is less likely to be managed in a PAS center with a multidisciplinary team, where specialized care may lower maternal morbidity and mortality21). As a result, despite the lesser degree of placental invasion, worse obstetric outcomes could occur in “unexpected PAS” compared to “expected PAS”6). Therefore, in a clinical setting, paying careful attention to pregnant women at risk of unexpected PAS is essential4). Kyozuka et al. reported that repeated cesarean sections in ART pregnancies are strongly associated with unexpected PAS4). Therefore, we introduced REBOA in Case 1, where the patient had a suspected CSP, to control obstetric bleeding. CSP, which is defined as a gestational sac implant at a previous myometrium scar due to cesarean section, is a rare form of ectopic pregnancy, accounting for 6.1% of ectopic pregnancies and 0.15% of pregnancies in women who have previously undergone cesarean section22,23). In most cases, CSP is diagnosed between 6 and 8 weeks of gestation when the gestational sac is clearly visible on ultrasound24). Because CSP is rare, accurate diagnosis of CSP after the second trimester is challenging if there is no evidence of placenta previa7). CSP without placenta previa sometimes presents as an unexpected PAS at the time of laparotomy. Suzuki et al. reported a case of unexpected PAS in a patient with CSP that required emergent cesarean hysterectomy by a multidisciplinary emergent team because of severe abnormal placental implantation. However, Case 2 showed no evidence of placenta previa on transvaginal ultrasound during perinatal care. CSPs are divided into two types based on imaging presentation and progression25). In type 1 (endogenic CSP), the gestational sac grows toward the uterine cavity, while in type 2 (exogenic CSP), the gestational sac grows toward the bladder. In a previous study, the diagnosis of type 1 CSP was delayed, and emergent cesarean hysterectomy by a multidisciplinary emergent team was needed because of unexpected PAS, which usually necessitates an immediate cesarean hysterectomy7). In contrast, type 2 CSP could develop as placenta previa and be diagnosed as conventional PAS, which allows enough time to set up a multidisciplinary medical team. As shown in Case 2, once the obstetric care provider suspects type 1 CSP, immediate transfer to a multidisciplinary medical center is reasonable due to the high risk of massive PPH or emergent cesarean hysterectomy7).
Future challenges
REBOA increases proximal blood pressure through aortic occlusion. However, because this occlusion induces distal ischemia of the visceral organs and lower extremities, which causes inflammatory sequelae and may be life-threatening or limb-threatening26), the attending physician should take the benefits and risks of REBOA into consideration. In addition, REBOA may lead to complications of organs proximal to the occlusion due to increased blood flow. Uchino et al. reported the case of an 86-year-old woman with fatal massive intracranial hemorrhage because of increased proximal blood flow using REBOA during the management of a severe pelvic fracture27). Cognizant of these physiological changes during the REBOA procedure, our institution excluded patients with hypertensive disorders of pregnancy, such as new onset hypertension after 20 weeks of gestation, from REBOA due to the potential risk of brain hemorrhage28) due to the increased blood flow resulting from REBOA.
Furthermore, because the terms “REBOA” and “Unexpected PAS” are still not commonly encountered among obstetricians, we thought that multidisciplinary simulation and prophylactic application of REBOA to cases with unexpected PPH in addition to conventional PAS may be essential for gaining expertise in REBOA.
In conclusion, we have introduced REBOA as a multidisciplinary medical procedure for cases with suspected unexpected PAS. Future collaborative studies should be performed in centers with multidisciplinary management protocols for highly suspect to unexpected placenta PAS to ensure better understanding of the characteristics and outcomes of the disease.