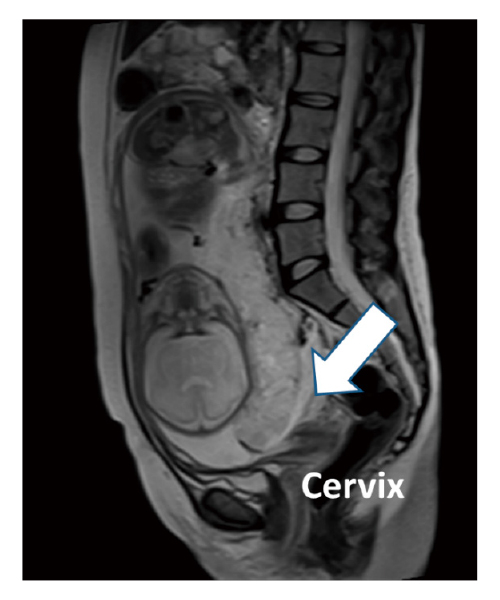
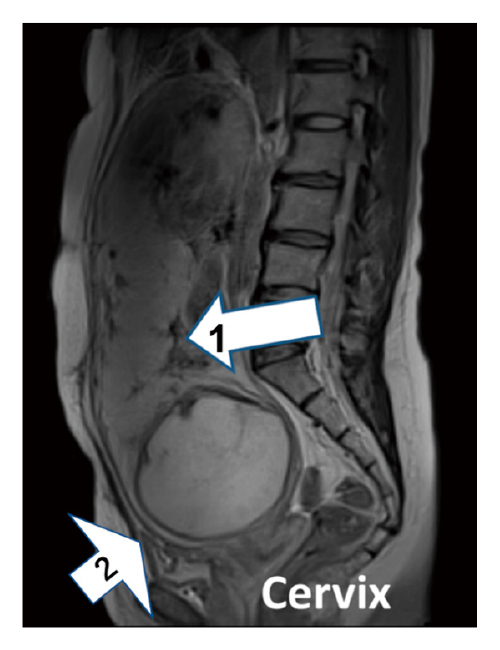
Postpartum hemorrhage is an important obstetric complication and the leading cause of maternal mortality worldwide. Occasionally, we encounter unexpected massive postpartum hemorrhage diagnosed for the first time after delivery. Therefore, it is essential to pay attention to patients with a high risk of postpartum hemorrhage. The authors report two cases of patients at high risk of postpartum hemorrhage that were successfully managed by resuscitative endovascular balloon occlusion of the aorta before cesarean section. Case 1: A 32-year-old woman with a history of cesarean section and who conceived using assisted reproductive technology was diagnosed with partial placenta previa at 25 weeks of gestation. Because of tocolysis failure, emergent cesarean section with resuscitative endovascular balloon occlusion of the aorta was performed at 36 weeks of gestation. Natural placental resorption was observed. She was discharged at 5 days after delivery without significant hemorrhage. Case 2: A 41-year-old woman with suspected placenta accreta spectrum due to a cesarean scar pregnancy was referred to our hospital at 33 weeks of gestation. A planned cesarean section with resuscitative endovascular balloon occlusion of the aorta was conducted at 37 weeks of gestation. There was no visual evidence of abnormal placental invasion of the myometrium, and natural placental resorption was observed. She was discharged at 5 days after delivery without significant hemorrhage.
Abstract/References
Introduction and utility of resuscitative endovascular balloon occlusion of the aorta for cases with a potential high risk of postpartum hemorrhage: A single tertiary care center experience of two cases
Hyo Kyozuka, Misa Sugeno, Tsuyoshi Murata, Toki Jin, Fumihiro Ito, Yasuhisa Nomura, Takaki Hirano, Kazuaki Shinohara, Daisuke Suzuki, Tokiya Ishida
-
Hyo Kyozuka
Department of Obstetrics and Gynecology, Ohta Nishinouchi Hospital
-
Misa Sugeno
Department of Obstetrics and Gynecology, Ohta Nishinouchi Hospital
-
Tsuyoshi Murata
Department of Obstetrics and Gynecology, Shirakawa Kosei General Hospital
-
Toki Jin
Department of Obstetrics and Gynecology, Ohta Nishinouchi Hospital
-
Fumihiro Ito
Department of Obstetrics and Gynecology, Ohta Nishinouchi Hospital
-
Yasuhisa Nomura
Department of Obstetrics and Gynecology, Ohta Nishinouchi Hospital
-
Takaki Hirano
Department of Emergency and Critical Care, Ohta Nishinouchi Hospital
-
Kazuaki Shinohara
Department of Emergency and Critical Care, Ohta Nishinouchi Hospital
-
Daisuke Suzuki
Department of Obstetrics and Gynecology, Ohta Nishinouchi Hospital
-
Tokiya Ishida
Department of Emergency and Critical Care, Ohta Nishinouchi Hospital
Abstract
References
1. Thurn L, Wikman A, Westgren M, Lindqvist PG. Massive blood transfusion in relation to delivery:Incidence, trends and risk factors:A population-based cohort study. BJOG, 126:1577-1586, 2019.
3. Kramer MS, Berg C, Abenhaim H, et al. Incidence, risk factors, and temporal trends in severe postpartum hemorrhage. Am J Obstet Gynecol, 209:449.e1-449.e7, 2013.
12. Della Torre M, Kilpatrick SJ, Hibbard JU, et al. Assessing preventability for obstetric hemorrhage. Am J Perinatol, 28:753-760, 2011.
14. Zhou T, Lu W, Wang W, et al. The Efficacy and Postoperative Follow-Up of Different Interventional Methods in Cesarean Section for Placenta Accreta Spectrum Disorders. Med Sci Monit, 27:e932674, 2021.
19. Paull JD, Smith J, Williams L, Davison G, Devine T, Holt M. Balloon occlusion of the abdominal aorta during caesarean hysterectomy for placenta percreta. Anaesth Intensive Care, 23:731-734, 1995.
20. Theodorou CM, Rinderknecht TN, Girda E, Galante JM, Russo RM. Fetal and Neonatal Outcomes Following Maternal Aortic Balloon Occlusion for Hemorrhage in Pregnancy:A Review of the Literature. J Trauma Acute Care Surg, 92:e10-e17, 2021.
21. Meller CH, Izbizky GH, Otaño L. Outcomes of Planned Compared With Urgent Deliveries Using a Multidisciplinary Team Approach for Morbidly Adherent Placenta. Obstet Gynecol, 131:1164-1165, 2018.
24. Kaelin Agten A, Cali G, Monteagudo A, Oviedo J, Ramos J, Timor-Tritsch I. The clinical outcome of cesarean scar pregnancies implanted “on the scar” versus “in the niche”. Am J Obstet Gynecol, 216:510.e1-e6, 2017.
26. Matsumura Y, Higashi A, Izawa Y, et al. Organ ischemia during partial resuscitative endovascular balloon occlusion of the aorta:Dynamic 4D Computed tomography in swine. Sci Rep, 10:5680, 2020.
27. Uchino H, Tamura N, Echigoya R, et al. “REBOA”- Is it really safe? A case with massive intracranial hemorrhage possibly due to endovascular balloon occlusion of the aorta (REBOA). Am J Case Rep, 1:810-813, 2016.
Figures (4)