

Metaiodobenzylguanidine (MIBG) accumulates in tumors derived from the adrenal medulla and sympathetic ganglia, and is useful in the localization of pheochromocytoma, neuroblastoma, medullary thyroid carcinoma, and carcinoid. To date, there have been few reports of MIBG accumulation in gastrointestinal stromal tumors (GISTs). We herein report and discuss three cases of MIBG accumulation in GISTs.
The content of research paper
Three cases of gastrointestinal stromal tumors with metaiodobenzylguanidine (MIBG) accumulation
Honami Kobiyama, Shiro Ishii, Yumi Saito, Natsumi Kawamoto, Shigeyasu Sugawara, Hiroshi Ito
Author information
-
Honami Kobiyama
Department of Radiology and Nuclear Medicine, Fukushima Medical University
-
Shiro Ishii
Department of Radiology and Nuclear Medicine, Fukushima Medical University
-
Yumi Saito
Department of Radiology and Nuclear Medicine, Fukushima Medical University
-
Natsumi Kawamoto
Department of Radiology and Nuclear Medicine, Fukushima Medical University
-
Shigeyasu Sugawara
Department of Radiology and Nuclear Medicine, Fukushima Medical University
-
Hiroshi Ito
Department of Radiology and Nuclear Medicine, Fukushima Medical University
Introduction
Case1
A 63-year-old male had a submucosal tumor of the stomach identified through a regular health check that included an upper gastrointestinal examination. Computed tomography (CT) was performed and a left adrenal tumor was suspected (Fig. 1a). Magnetic resonance imaging (MRI) was performed for detailed examination. T1-weighted imaging (T1WI) showed a well-defined mass in contact with the gastric wall with no obvious fat content (Figs. 1b, 1c). The mass showed high signal intensity on diffusion-weighted imaging (DWI, Fig. 1d). The tumor seemed to be separated from the left adrenal gland, but paraganglioma was not ruled out. Posterior view of I-123 MIBG scintigraphy showed normal accumulation in the bilateral adrenal glands and abnormal accumulation in the left upper abdomen (Figs. 2a, 2b, black arrows).
Urinary catecholamine levels were within normal limits, indicating a low likelihood of functioning paraganglioma.
Subepithelial lesions on the upper posterior wall of the gastric body were found via endoscopy. They were difficult to identify in white light; however, they were confirmed by endoscopic ultrasound (EUS), which showed a hypoechoic mass with internal heterogeneity in the fourth layer (Figs. 2c, 2d).
The patient underwent laparoscopic and endoscopic cooperative surgery (LECS) for tumor resection. The tumor contained bundles of spindle cells. Immunostaining showed positive reactivity for CD117, CD34, and caldesmon, as well as negative reactivity for S-100, leading to a diagnosis of GIST.
The patient received imatinib mesilate 300 mg as postoperative chemotherapy for about 3 years, and showed no recurrence in subsequent examinations.
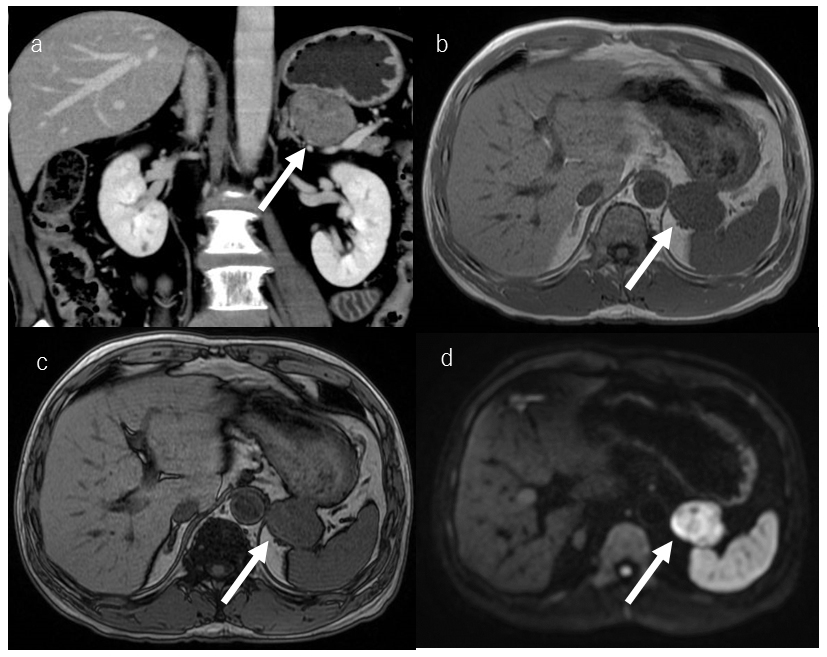
Fig. 1.
Coronal image of contrast-enhanced CT (a) showed a tumor near the left adrenal gland (white arrow). In-phase (b) and out-of-phase T1WI (c) showed a well-defined mass in contact with the gastric wall, with no obvious fat content (white arrows). The mass showed high signal intensity DWI (d, white arrow).
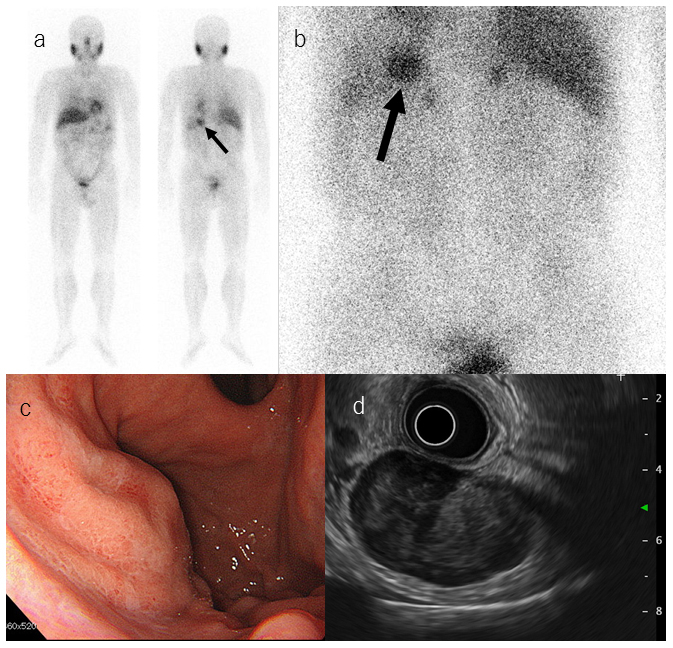
Fig. 2.
An abnormal accumulation in the left upper abdomen was observed in I-123 MIBG scintigraphy (a, b, black arrows).
Endoscopic images of subepithelial lesions on the posterior wall of the upper gastric body, confirmed by EUS, which shows a hypoechoic mass with internal heterogeneity in the fourth layer (c, d).
Case 2
A 76-year-old female with a medical history of hypertension had abdominal discomfort, loss of appetite, and weight loss. Upper gastrointestinal endoscopy revealed an indentation in the upper part of the gastric body. Abdominal CT showed marked thickening of the gastric wall, suggesting leiomyosarcoma.
For further investigation, contrast-enhanced computed tomography (CECT) was performed and showed a huge mass with internal necrosis in the left upper abdomen (Fig. 3a, white arrows). The tumor was thought to be derived from the gastric serosa or mesentery. The spleen was infiltrated; however, with no enlargement of lymph nodes and a small amount of ascites, neither dissemination nor metastasis was suspected. I-123 MIBG scintigraphy, performed to rule out pheochromocytoma before biopsy, showed a strong accumulation in the lesion on the anterior image (Figs. 3b, 3c, black arrows). Urinalysis and blood tests showed no findings suspicious for a functioning pheochromocytoma.
No tumor exposure or wall thickening was observed via endoscopy with normal light but an extensive mass with necrosis was observed outside the gastric wall, and suspected hepatic infiltration was detected via an upper gastrointestinal endoscopic ultrasound (EUS, Fig. 3d). EUS-guided fine needle aspiration (EUS-FNA) was also performed, and showed spindle cells. Immunostaining showed positive reactivity for CD117, CD34, and caldesmon, but negative reactivity for desmin and S-100 protein. The pathological diagnosis was GIST.
Since the tumor was large and infiltration of surrounding organs was observed, it was decided to operate after chemotherapy. Initially, the tumor showed a tendency to shrink by imatinib mesilate 300 mg, but one nodule of the tumor increased in size. Treatment was continued by changing to sunitinib, but the tumor was enlarged. The patient died after 3 years in palliative care.
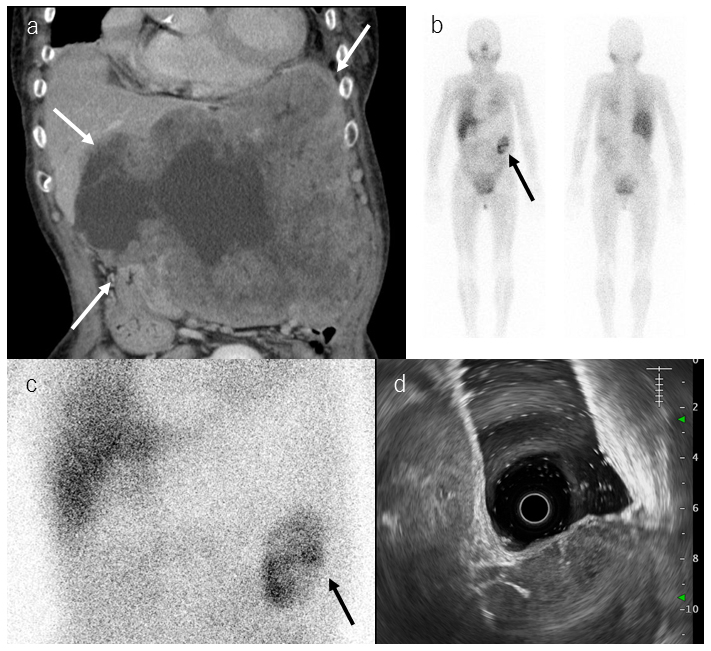
Fig. 3.
Coronal contrast-enhanced CT showed a huge mass with internal necrosis in the left upper abdomen (a, white arrows). Anterior image of I-123 MIBG scintigraphy showed a strong but partial accumulation in the mass (b, c, black arrows).
The mass was seen outside the gastric wall and hepatic infiltration was suspected by an upper gastrointestinal EUS (d).
Case 3
A 51-year-old male was found to have a small gastric submucosal tumor by endoscopy at his previous hospital, and was followed by observation. Four years later, the tumor increased in size, and GIST was suspected by CT.
CT showed a tumor protruding outside the lateral wall of the gastric lesser curvature and bilateral adrenal nodules were noted. MRI and I-131 MIBG scintigraphy were performed to rule out pheochromocytoma. The gastric tumor had a low signal on T2-weighted imaging (T2WI, Fig. 4a, white arrow) and fatty bilateral adrenal nodules seen on MRI were suspected to be adenoma. Anterior view of I-131 MIBG scintigraphy did not show abnormal accumulation in the bilateral adrenal glands, but a strong accumulation in the gastric tumor (Figs. 4d, 4e, black arrows). EUS revealed a hypoechoic mass with internal heterogeneity in the fourth layer, and the mass was suspected to infiltrate outside of the wall.
EUS-FNA was performed, revealing spindle cells. Immunostaining showed positive reactivity for c-kit and CD34, but negative reactivity for desmin, S-100 protein, and SMA. Pathological diagnosis was gastric GIST. The tumor was considered to be a low-risk GIST because of the small number of mitotic Figs. (50 per high-power field), but it continued to grow, and partial gastrectomy and left adrenalectomy were performed. The size of gastric tumor was 4.5 × 3.6 × 4.5 cm. Since then, there has been no recurrence or metastasis of the GIST, and the right adrenal adenoma has been under observation.
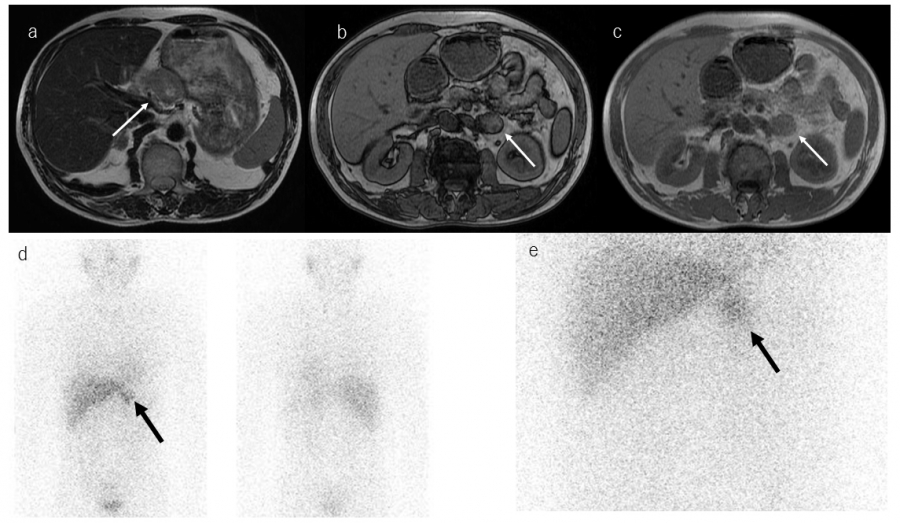
Fig. 4.
Axial T2WI showed the gastric tumor with mixed signal intensity (a, white arrow). The bilateral adrenal nodules had lower signal intensity on out-of-phase images (b, white arrow) than in-phase images (c, white arrow), indicating adrenal adenoma (only the left side mass is presented).
I-131 MIBG scintigraphy did not show abnormal accumulation in the bilateral adrenal glands, but showed a strong accumulation in the gastric tumor, anterior view (d, e, black arrows).
Discussion
MIBG is an analog of noradrenaline and guanethidine, specifically taken up by adrenergic neurons via norepinephrine transporter uptake-1, and stored in catecholamine storage granules in sympathetic nerve terminals and adrenal medullary cells1,2). GISTs are interstitial tumors derived from interstitial cells of Cajal (ICC) that localize in the intermuscular plexus of the gastrointestinal wall2,3). MIBG scintigraphy is used to diagnose tumors derived from sympathetic nerves such as pheochromocytoma and paraganglioma, or to visualize cardiac sympathetic nerve activity, rather than to diagnose GIST.
MIBG scintigraphy was performed for the purpose of diagnosing or excluding pheochromocytoma in our three cases, and unexpected accumulation of MIBG in GIST was observed. To date, seven cases of GIST with MIBG accumulation including our own have been reported (Table)2,4,5,6). Balan et al. reported a patient with a history of pheochromocytoma who was diagnosed with Carney’s triad (pheochromocytoma, GIST, and pulmonary chondroma)6); however, the other six cases including ours were not associated with Carney’s triad and were of gastric GIST. This high frequency of gastric involvement is consistent with that of GIST as mentioned above. Among the seven cases, MIBG accumulation was observed throughout most of the tumors except for our case 2, in which partial tumor accumulation was observed. This might indicate heterogeneity or differentiation of GISTs. Although the exact mechanism of MIBG accumulation in GISTs remains unclear, Fukuchi et al. hypothesized two possibilities. First, ICCs have the capability to uptake MIBG2). Because ICCs have neuron-like characteristics that mediate neuronal input from the enteric nervous systems, they might have neurosecretory granules that uptake norepinephrine. Second, a special type of GIST called gastrointestinal autonomic nerve tumor (GANT) may be able to uptake MIBG2). GANT is known to have bulbous synapse-like structures containing clusters of dense core neurosecretory granules7,8), which may accumulate MIBG2). GANTs have been reported to be positive for vimentin, CD34, and NSE in an immunohistochemical study2).
When MIBG accumulates in an abdominal mass suspected to be a GIST, sometimes it is clinically important to differentiate GIST from pheochromocytoma and paraganglioma. Because about 10% of pheochromocytomas and paragangliomas are nonfunctional tumors and do not present with typical symptoms such as hypertension, palpitations, headache, and sweating4), asymptomatic pheochromocytoma cannot be ruled out.
Although the frequency and exact mechanism of MIGB accumulation in GISTs are yet unknown, several cases of GISTs with MIBG accumulation have been reported, and MIBG scintigraphy may be useful for their diagnosis. However, basic research, case-control studies, and further case collection are needed to elucidate the utility of MIBG imaging for GIST.
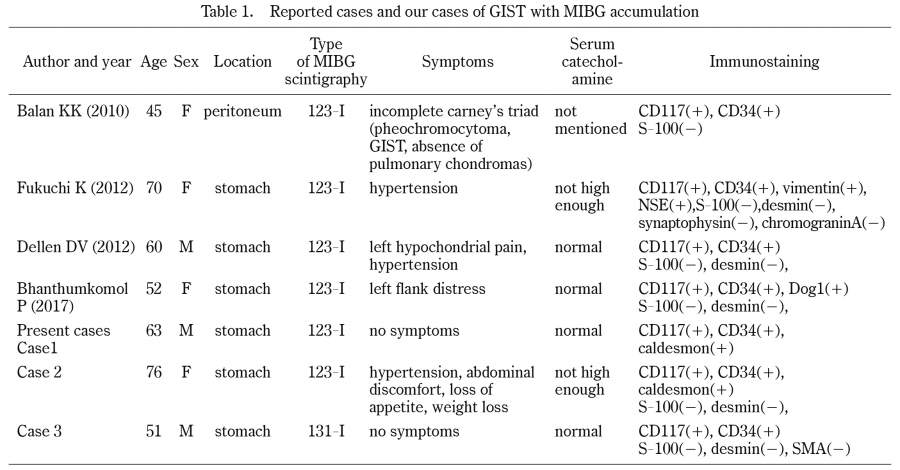
Table 1.
Reported cases and our cases of GIST with MIBG accumulation
Conclusion
MIBG can accumulate in GISTs, although the uptake mechanism remains unclear. When assessing tumors with MIBG accumulation, GIST should be included in the differential diagnosis.