M2 inhibitor
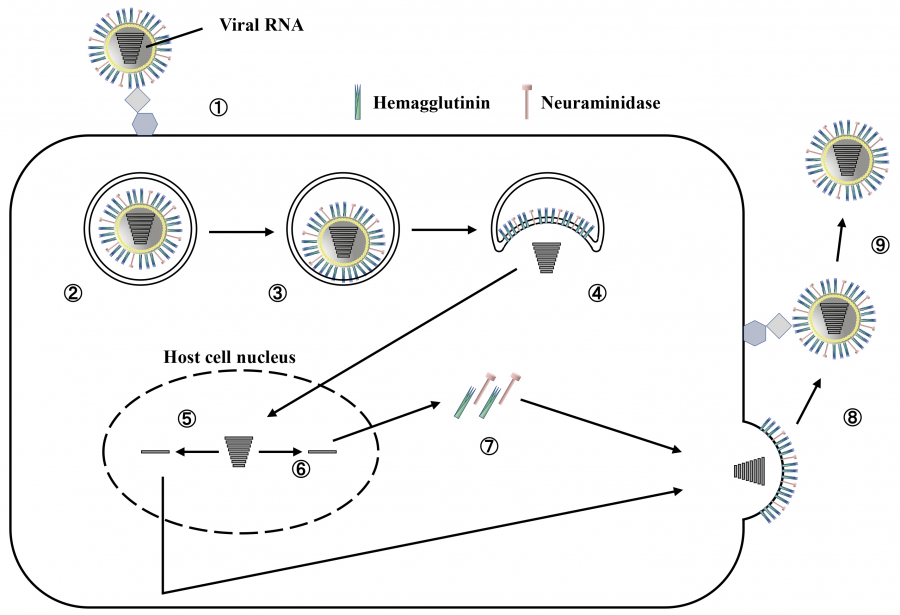
The type A virus has an ion channel formed by the M2 protein, and when outside hydrogen ions enter the virus through this channel, uncoating occurs.
Amantadine, an M2 inhibitor, exhibits antiviral effects by targeting this M2 protein ion channel and inhibiting uncoating. This drug has been used in the United States and other countries since the 1960s. However, most type A viruses isolated today are resistant to amantadine6), and type B viruses do not have the M2 protein, making amantadine ineffective. Thus, M2 inhibitors are not currently administered.
NA inhibitors
As described above, to release the replicated progeny virus from the cell surface, HA must be detached from sialic acid using the sialic acid–degrading enzymatic activity of NA (Figure 1). Current NA inhibitors prevent the enzymatic activity of sialic acid–based degrading enzymes. In other words, NA inhibitors are enzyme inhibitors. In the 1970s, the sialic acid derivative 2,3-dehydro-2-deoxy-N-acetylneuraminic acid (DANA) was reported to inhibit NA activity7). Subsequently, based on the DANA structure, a computer-aided drug design led to the development of drugs that inhibit NA activity more potently. Thus, current NA inhibitors, such as oseltamivir, zanamivir, laninamivir, and peramivir, are DANA derivatives, and their analogs exhibit similar structures (Figure 2).
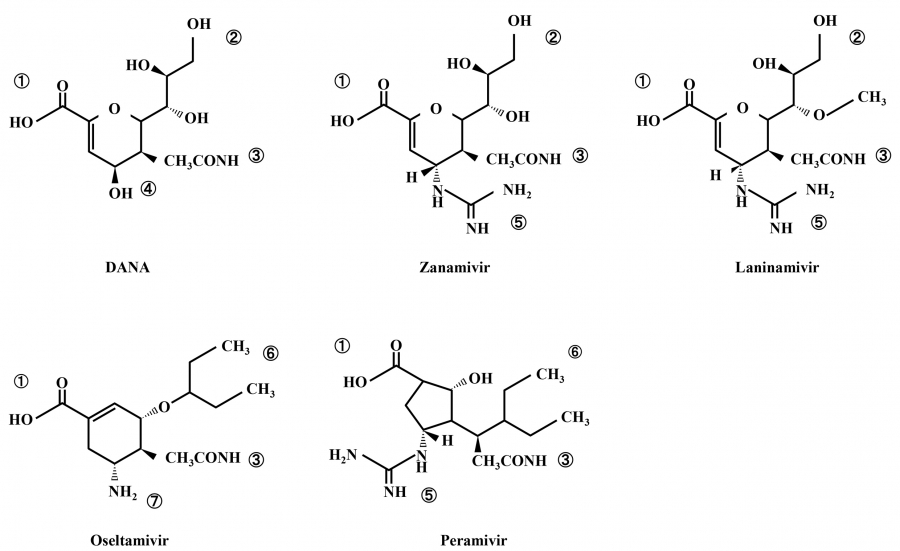
Fig. 2.
Structure of neuraminidase inhibitors
① carboxyl group, ② glycerol group, ③ N-acetylamino group, ④ hydroxy group, ⑤ guanidino group, ⑥ 3-pentyl group, and ⑦ amino group
DANA, 2,3-dehydro-2-deoxy-N-acetylneuraminic acid
Oseltamivir
Oseltamivir is available in two dosage forms:75 mg capsules and 3% dry syrup. It has been approved for use in the treatment of influenza and as a post-exposure prophylaxis regimen (Table 1).
The active form of oseltamivir (oseltamivir carboxylate) has low bioavailability when administered orally8); hence, the precursor oseltamivir phosphate is administered orally, which is then converted into the active form in the body. In adults, when 75 mg per dose oseltamivir is administered orally, the maximum plasma concentration of the active form of the drug is approximately 1200 nM. However, because children have higher extracellular fluid per body weight and larger volume of distribution, as well as the higher clearance rate of the active form per body weight is inversely proportional to age9,10), the maximum plasma concentrations of the active form is approximately 700 nM in children aged 9–12 years and 400 nM in those aged 1–2 years, with lower concentrations in younger age groups11). As influenza viruses infect and multiply in the airways, the extent to which the active form is transferred from the blood to the airways is a more significant issue than the blood drug concentration. In animal models, the highest concentration of the active form in the airways is ~70% of the highest plasma concentration12); however, its concentration in the human lower respiratory tract remains unknown. In human saliva, the concentration of the active form is ~5% of the plasma concentration13); nonetheless, it is considerably higher than 50% of the inhibitory concentration (IC50) (Table 2)14). If the NA activity of susceptible type A virus is inhibited by 50%, a sufficient effect is expected.
In adults, oseltamivir has been demonstrated to shorten the symptomatic period and prevent complications compared with placebo15). In fact, during the H1N1 pdm09 epidemic, which caused many deaths worldwide, the oseltamivir group had a significantly lower mortality rate than the untreated group16). In children, the febrile period was reduced by approximately 25 h in the oseltamivir group compared with that in the placebo group; consequently, complications such as otitis media were controlled, and unnecessary administration of antimicrobial agents was prevented17). A retrospective cohort study involving critically ill children who were systemically managed in an intensive care unit (ICU) showed that oseltamivir administration within 24 h of ICU admission contributed to reducing hospitalization duration compared with no oseltamivir treatment18). In Japan, compared with children not treated with oseltamivir, the fever duration in type A (H3N2) and type B influenza was reduced by approximately 20 h in children treated with oseltamivir19). However, patients treated with oseltamivir showed no reduction in the infectious virus shedding period compared with those who were not treated with oseltamivir, and infectious viruses continued shedding for 5–7 days after the onset of illness19). Based on this previous report, the duration of suspension from school or preschool after the onset of influenza has been established by law in Japan. Both oseltamivir and zanamivir are equally effective in reducing fever duration in type A influenza; however, in type B influenza, oseltamivir is less effective than zanamivir in reducing fever duration20,21). Oseltamivir can rotate the NA active center (E276) and induce a hydrophobic pocket with R224, binding to that site via a 3-pentyl group (Figures 2 and 3)22-24). However, compared with type A virus, E276 rotation is less likely to occur in type B virus. Therefore, the hydrophobic pocket accommodating the 3-pentyl group is not induced25), and the IC50 value of oseltamivir for type B viruses is higher than that for type A viruses (Table 2)14). Consequently, the clinical efficacy of oseltamivir against type A influenza differs from that against type B influenza.
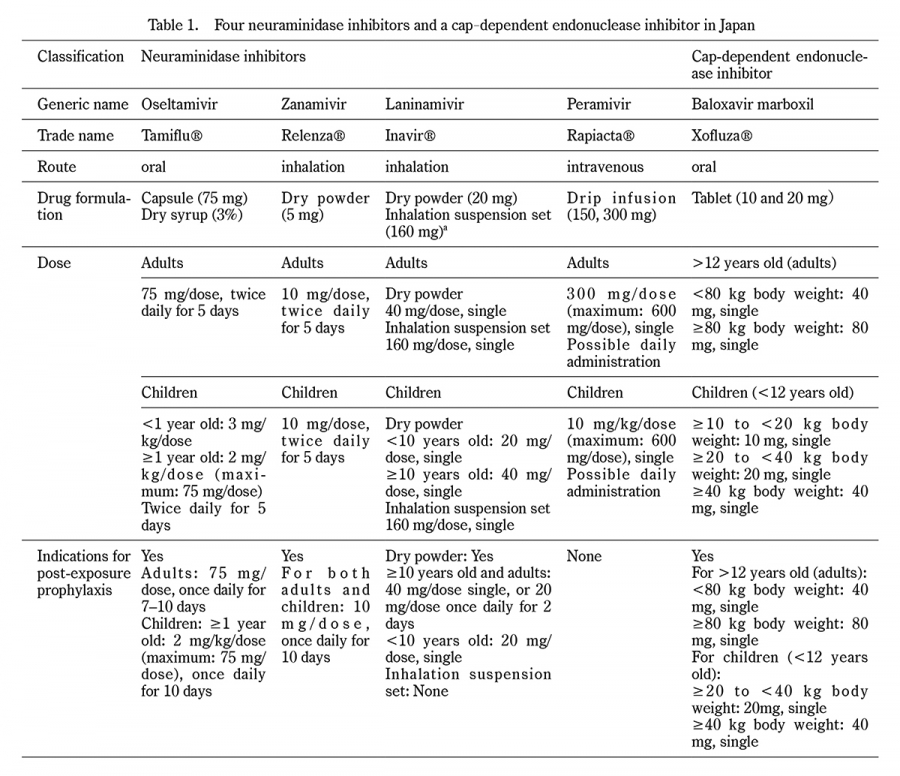
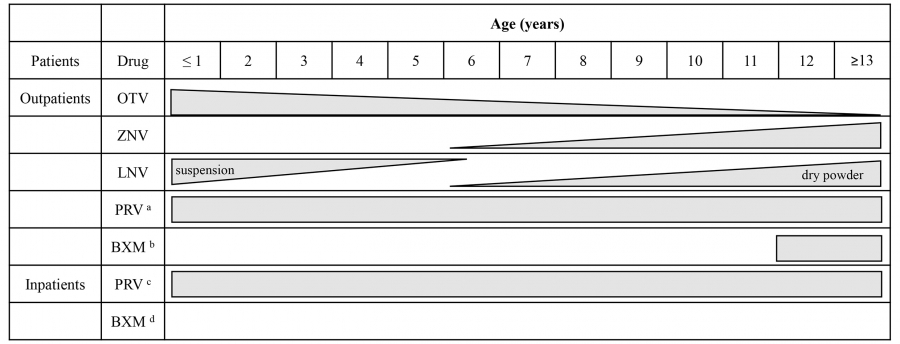
Table 1.
Four neuraminidase inhibitors and a cap-dependent endonuclease inhibitor in Japan
*a, a jet nebulizer required
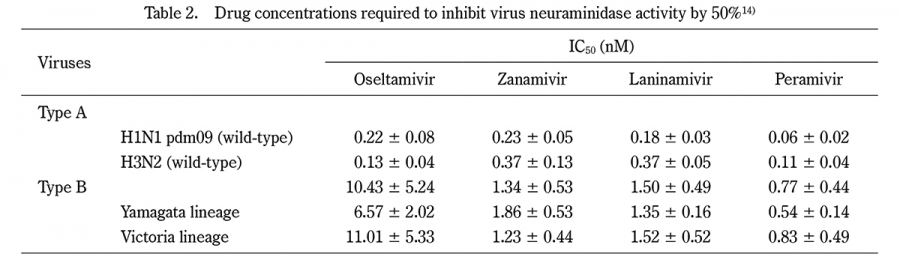
Table 2.
Drug concentrations required to inhibit virus neuraminidase activity by 50%14)
Mean ± standard deviation
IC50: 50% of inhibitory concentration
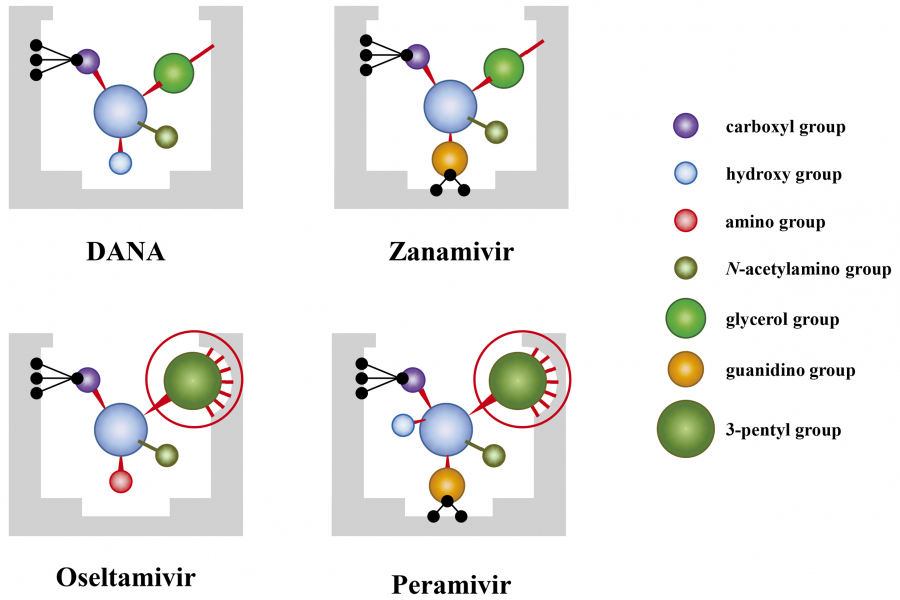
Fig. 3.
Binding of drugs to virus neuraminidase
Each neuraminidase inhibitor binds to the active site of viral neuraminidase (gray solid) using its side chain. Oseltamivir and peramivir are required to induce the formation of hydrophobic pockets (red circle) on the viral neuraminidase for successful binding. DANA, 2,3-dehydro-2-deoxy-N-acetylneuraminic acid
Zanamivir and laninamivir
Given that influenza spreads and multiplies in the airways, the concentration of antiviral drugs in the airways should be high. The inhalants zanamivir and laninamivir are the most reasonable agents. Both drugs have been approved for influenza treatment and post-exposure prophylaxis (Table 1).
When zanamivir is inhaled, most of the drug is distributed from the posterior pharyngeal wall to the larynx, with only approximately 15% reaching the lower respiratory tract; nevertheless, more than 3000 nM of the drug is still thought to remain in the airways 6 h after inhalation26). The IC50 values for zanamivir against type B virus are lower than those of oseltamivir (Table 2)14). As mentioned above, its clinical efficacy is higher than that of oseltamivir20,21,27), and the duration of virus shedding tends to be shorter in children19). The structure of laninamivir is very similar to that of zanamivir (Figure 2); both drugs also have a similar inhibitory effect on NA activity (Table 2)14). Given that zanamivir is water-soluble, its clinical efficacy was also confirmed in children by dissolving it in saline or other solutions and inhaling it using a nebulizer19), but this inhalation method using a zanamivir solution is not currently approved.
Meanwhile, laninamivir inhales its precursor called laninamivir octanoate, which is fat-soluble, allowing it to enter the cells in the airways, where it is hydrolyzed into the active form in the cells. Therefore, laninamivir is believed to bind to NAs intracellularly, whereas other NA inhibitors inhibit viral NAs extracellularly. Furthermore, considering that laninamivir has a long half-life in the airways of approximately 41 h28), a single inhalation is sufficient to complete the treatment.
In noninferiority studies involving patients treated with laninamivir and oseltamivir in Japan and other Asian countries, the clinical efficacy of laninamivir was not inferior to that of oseltamivir29,30). Another noninferiority study investigating pediatric patients during an oseltamivir-resistant virus epidemic in Japan showed that laninamivir significantly reduced the duration of symptoms compared with oseltamivir31). These findings led to the approval of laninamivir use in Japan.
However, laninamivir is not approved in the United States because of the lack of clinical efficacy in a double-blind, placebo-controlled study32).
In children, the inhalation dose differs between those younger and older than 10 years (Table 1). Of note, even children younger than 10 years may not receive a sufficient dose, depending on their size. When laninamivir can be successfully inhaled in children, its clinical efficacy may be equivalent to that of zanamivir inhalation for five days33). When comparing the clinical efficacy of laninamivir with that of zanamivir (both are inhaled drugs), laninamivir is associated with more recurrent fever in younger age groups34), possibly because it is a single-inhalation complete drug, whereas zanamivir can be inhaled twice daily for five days. Therefore, zanamivir or oseltamivir should be considered when full inhalation of laninamivir cannot be assured. In 2019, an inhaled suspension formulation of laninamivir was launched to allow younger children to inhale this drug. However, the administration of this new formulation has not been reported because of the outbreak of the novel coronavirus infection shortly after.
Peramivir
Peramivir is currently the only intravenous formulation of NA inhibitors; it has the advantage of ensuring that the target dose is administered in patients with an available intravenous route. This drug binds more strongly to viral NA than oseltamivir and might inhibit NA activity for a relatively longer time35). In mild influenza cases, a single once-daily dose of peramivir is sufficient to achieve clinical efficacy. However, peramivir has not yet been approved for use as a post-exposure prophylaxis regimen.
A single intravenous dose of 300 mg of peramivir in adults reportedly provides sufficient effective concentrations in the upper and lower respiratory tracts36), facilitating earlier resolution of fever and shorter symptomatic periods than the placebo group37). Furthermore, in hospitalized cases, its clinical efficacy is comparable to that of oseltamivir38). A single 10 mg/kg dose of peramivir in children has been shown to reach a maximum concentration of 5000 nM in the airways (Figure 4)39) with clinical efficacy39,40). For type A virus, the viral load after 1 or 2 days of administration can be reduced to <1% of the pre-dose level39). Compared with oseltamivir and zanamivir39,41), peramivir may reduce the viral load earlier, although making a general comparison is not possible because the studies were not conducted concurrently. However, in infants, peramivir is excreted from the respiratory tract approximately 35 h after administration (Figure 4)39). Therefore, in some children, type A virus may reappear 72 h after peramivir administration; moreover, infectious virus has been isolated in 50% of these children with viral reappearance39). For the type B virus, the viral load cannot be sufficiently reduced even on the day following peramivir administration39), possibly because peramivir concentrations in the blood and airways decrease rapidly immediately after administration39). Regarding peramivir, the IC50 value for type B virus is higher than that for type A virus (Table 2)14).
Because peramivir concentration in the blood decreases rapidly after administration, peramivir can be administered repeatedly regardless of age. However, in patients with impaired renal function, the decrease in blood peramivir concentration is slower; thus, the dosage should be adjusted accordingly42).
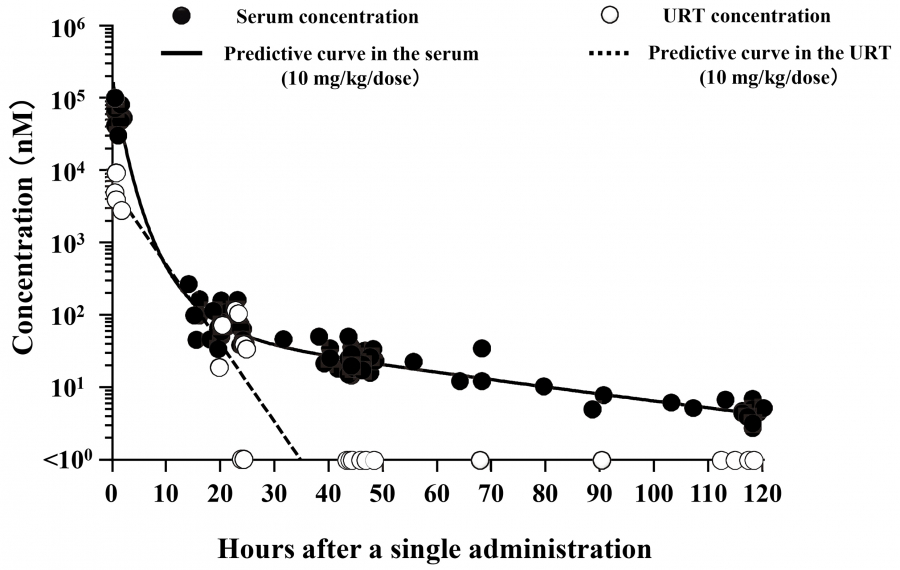
Fig. 4.
Peramivir concentration after a single intravenous administration
After a single administration of peramivir, a maximum concentration of 5000 nM of peramivir in the URT is expected, but in children, this drug may be eliminated from the URT approximately 35 h after administration39). URT, upper respiratory tract.
CEN inhibitor
As described in the section on the life cycle of influenza, influenza viruses utilize the CEN activity of the RNA polymerase PA subunit of the virus itself to cut out approximately 15 bases from the host-derived mRNA with a cap structure at the 5′-end. These short bases are used as a primer to transcribe the genetic information from the viral negative-stranded RNA to mRNA and synthesize viral proteins. The drug baloxavir inhibits this CEN activity43). It inhibits the transcription of viral RNA to mRNA, thereby reducing viral protein synthesis. Considering that current NA inhibitors prevent the release of replicated progeny from infected cells, baloxavir may reduce viral load in the early infection stages even more than NA inhibitors. In fact, compared with oseltamivir-treated patients, baloxavir-treated patients showed significantly lower viral load immediately after administration44). Therefore, it was expected that patients treated with baloxavir would recover from clinical symptoms earlier than those treated with oseltamivir, but no significant difference in symptomatic time was observed between these two patient groups44). The indication for prophylactic dosing has been approved for baloxavir because of its ability to suppress infection spread within the family, according to the early post-dose decrease in viral load45).
However, some variants with reduced susceptibility to baloxavir are detected after treatment in 20%–30% of children receiving this drug46-48). A higher percentage of these variants are detected in the A/H3 subtype than in the A/H1 subtype46-48). In these cases, viral load re-increases, the viral shedding period lengthens46-48), and perhaps, the clinical symptom duration increases46-48). Baloxavir is marketed in 10 and 20 mg tablets, and although a 2% granule formulation is approved for production, it has not yet been marketed.