Table 2 shows the demographic characteristics and operative outcomes of the Upper -GI and Lower-GI groups. The Upper-GI group had significantly older patients, predominantly male, and more patients admitted to intensive care than the Lower-GI group. Cefazolin was frequently used as a prophylactic antibiotic in the Upper-GI group, whereas cefmetazole was frequently used in the Lower-GI group. There were no significant differences in comorbidities, steroid use, length of hospital stay, or hospital death between the two groups; however, the number of patients with a previous hospitalization was significantly higher in the Upper-GI group than in the Lower-GI group. Furthermore, the Upper-GI group had a higher percentage of patients requiring endotracheal intubation, central venous catheterization, and blood purification therapy than the Lower-GI group. A higher percentage of P. aeruginosa was isolated from sputum in the Upper-GI group, whereas a higher percentage ofP. aeruginosa was isolated from urine in the Lower-GI group.
The Upper-GI group had more cases with an IPM score of 4 or 5 (i.e. cases with a breakpoint of R as resistance to IPM) than the Lower-GI group, although there were no differences in either AMK or CPFX scores. The Upper-GI group had significantly higher MDRP scores than the Lower-GI group (Fig. 1). In addition, the Upper-GI group had higher meropenem (MEPM), doripenem (DRPM), and cefozopran (CZOP) scores than the Lower-GI group (Table 3).
Next, we investigated the antibiotic resistance according to the isolation sites in the two groups (Table 4). Among P. aeruginosa isolates from drain discharge, a significantly higher rate of resistance to IPM, AMK, CPFX, tazobactam/piperacillin (TAZ/PIPC), MEPM, DRPM, CZOP, and levofloxacin was observed in the Upper-GI group. Similarly, among P. aeruginosa isolates from wounds, a significantly higher proportion was resistant to IPM, PIPC, TAZ/PIPC, ceftazidime, and CZOP in the Upper-GI group. However, there was no difference between the two groups in the drug resistance of P. aeruginosa isolated from urine, sputum, blood, and ascites. P. aeruginosa isolated from sputum was more likely to show resistance to IPM (P=0.07) than that isolated from other sites (Fig. 2) and was more likely to have higher MDRP scores than that isolated from other sites, specifically there were significant differences compared to that from wound and ascites (Fig. 3).

Table 2.
Demographics and operative outcomes in the Upper-GI and Lower-GI groups
GI, gastrointestinal; IBD, inflammatory bowel disease; CEZ, cefazolin; CMZ, cefmetazole
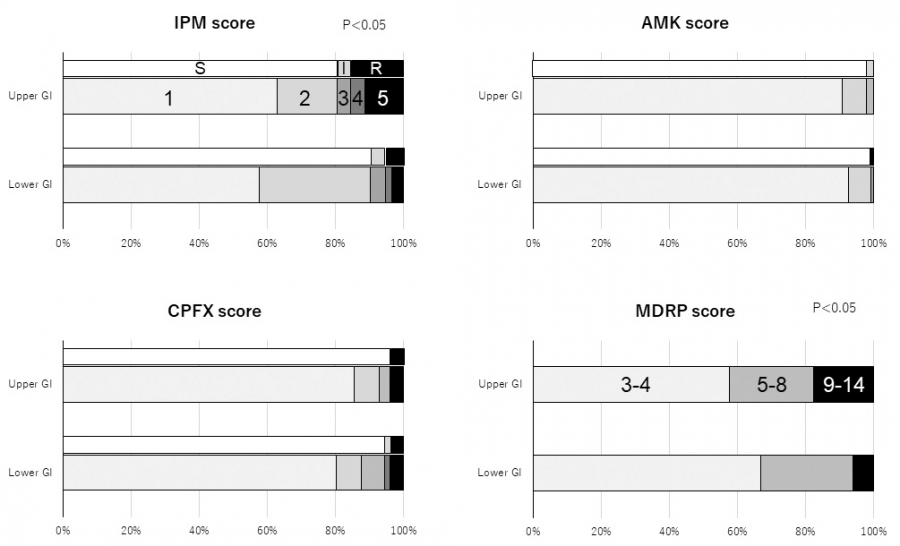
Fig. 1.
Susceptibility to three classes of antibiotics and MDRP scores in the Upper-GI and Lower-GI groups
The Upper-GI group had more cases with an IPM score of 4 or 5 (i.e. cases with a breakpoint of R as resistance to IPM) than the Lower-GI group, although there were no differences in either AMK or CPFX scores. The Upper-GI group had significantly higher MDRP scores than the Lower-GI group.
GI, gastrointestinal; IPM, imipenem; AMK, amikacin; CPFX, ciprofloxacin; MDRP, multidrug resistant-Pseudomonas aeruginosa

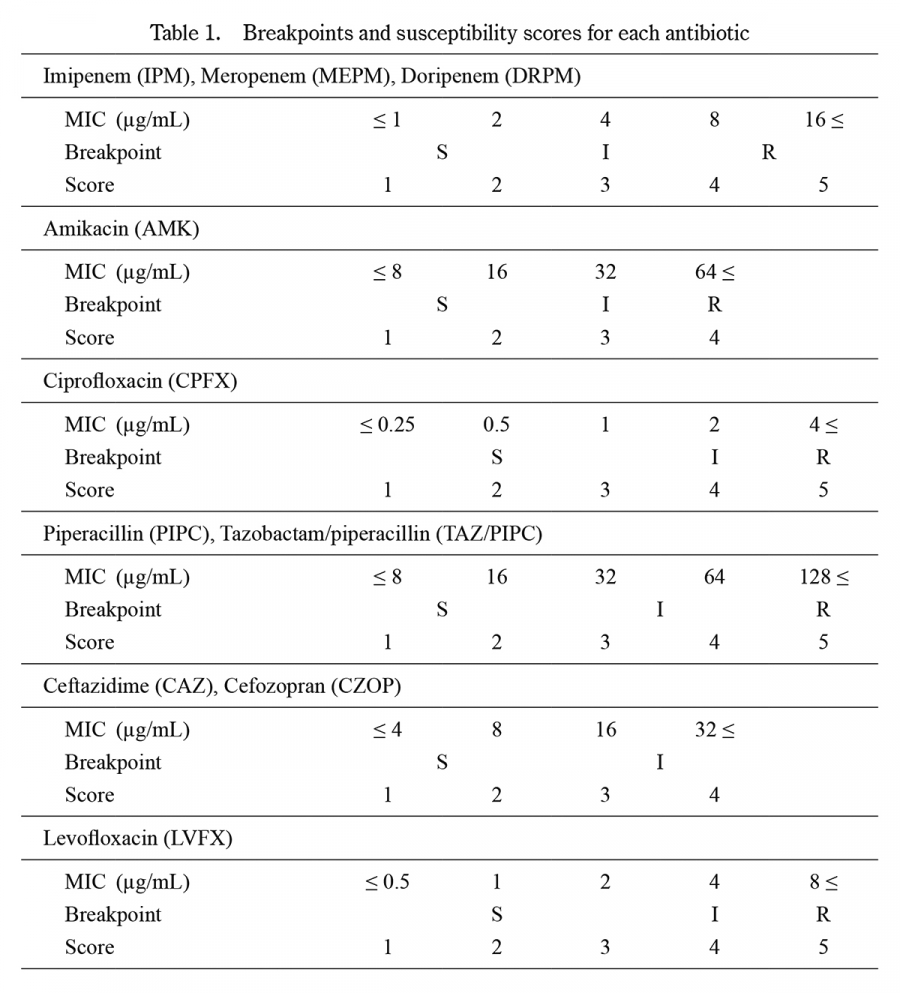
Table 3.
Breakpoints for antibiotics in the Upper-GI and Lower-GI groups
GI, gastrointestinal; PIPC, piperacillin; TAZ/PIPC, tazobactam/piperacillin; MEPM, meropenem; DRPM, doripenem; CAZ, ceftazidime; CZOP, cefozopran; LVFX, levofloxacin; NA, not assigned
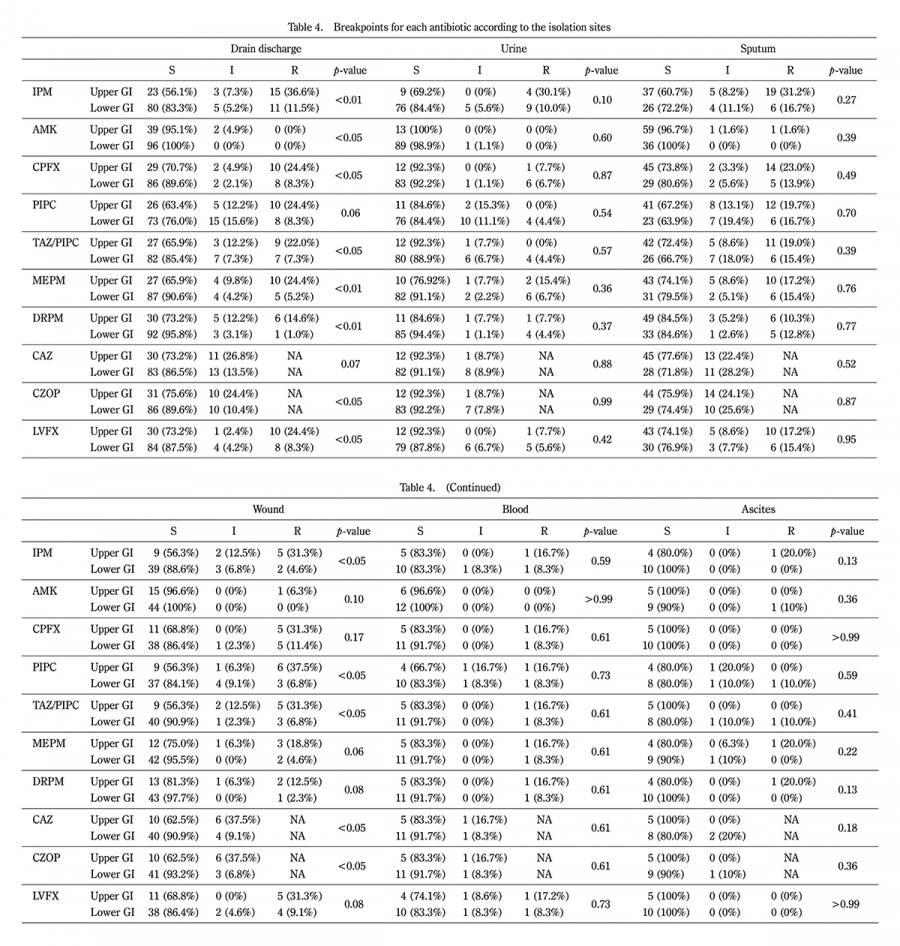
Table 4.
Breakpoints for each antibiotic according to the isolation sites
GI, gastrointestinal; IPM, imipenem; AMK, amikacin; CPFX, ciprofloxacin; PIPC, piperacillin; TAZ/PIPC, tazobactam/piperacillin; MEPM, meropenem; DRPM, doripenem; CAZ, ceftazidime; CZOP, cefozopran; LVFX, levofloxacin; NA, not assigned; S, susceptible; I, intermediate; R, resistant
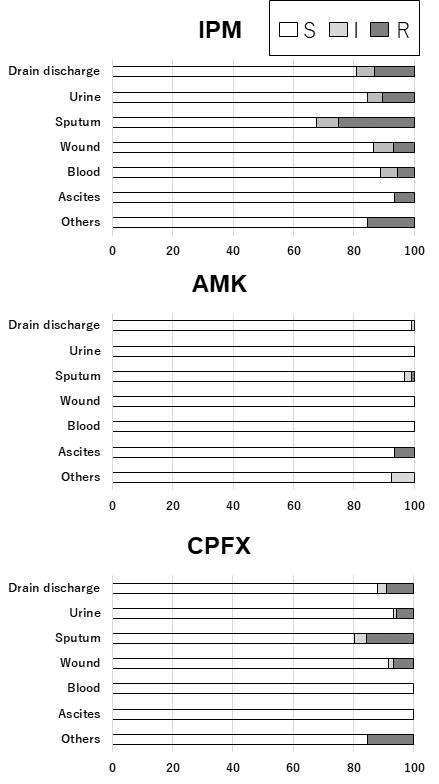
Fig. 2.
Breakpoints for IPM, AMK, and CPFX according to the isolation sites.
Pseudomonas aeruginosa isolated from sputum was more likely to show drug resistance to IPM and CPFX than those isolated from other sites.
IPM, imipenem; AMK, amikacin; CPFX, ciprofloxacin
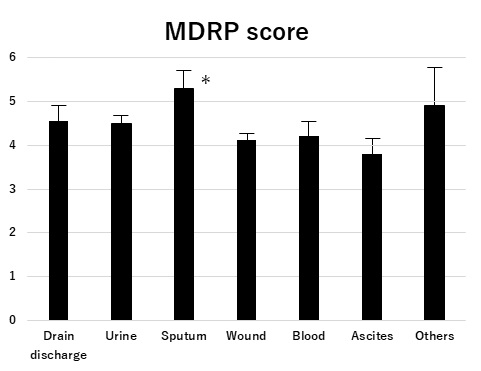
Fig. 3.
MDRP score according to the isolation sites
Pseudomonas aeruginosaisolated from sputum more likely had higher MDRP scores than those isolated from other sites.
*P< 0.05 versus wound and ascites
MDRP, multidrug resistant-Pseudomonas aeruginosa