PR3-ANCA and MPO-ANCA
AAV is characterized by systemic necrotizing vasculitis and patients fall into two groups:those with PR3-ANCA and those with MPO-ANCA. In the present study, all of our patients with AAV were MPO-ANCA positive, PR3-ANCA negative, and had effusion in the middle ear. In a report on the frequency of ear symptoms in the two groups, Nakamaru et al. reported that all patients with chronic otitis media were PR3-ANCA positive, whereas 89% of patients in the MPO-ANCA group had secretory otitis media4). Furthermore, previous studies reported that for GPA, the PR3-ANCA titer has 66% diagnostic sensitivity and MPO-ANCA has 24% sensitivity;for MPA, PR3-ANCA has 26% sensitivity and MPO-ANCA 50% to 80% sensitivity5,6).
Most patients (70-80%) with GPA are positive for PR3-ANCA and few (10%) are positive for MPO-ANCA, and it was reported that serum MPO-ANCA was positive in some patients with histopathologically diagnosed GPA7-10). Therefore, MPO-ANCA-positive middle ear disease should be classified as a subtype of GPA despite the lack of histopathological evidence of vasculitis.
Thus, elevation of PR3-ANCA or MPO-ANCA titer is one of the diagnostic criteria for AAV. In our study, all 7 cases with the disorder had ear symptoms that did not conform to the current Japanese diagnostic criteria.
Epidemiology
The epidemiology of systemic vasculitides differs between Japan, Europe, and North America11). For example, Takayasu’s arteritis occurs frequently and MPA- and MPO-ANCA-associated vasculitides are more common in Japan, while GPA- and PR3-ANCA-associated vasculitides are more common in the United Kingdom12).
Watanabe et al.13) reported that MPO-ANCA-related nephritis constitutes 60% of rapidly progressive glomerulonephritis (RPGN) cases in Japan. In a previous study comparing patient backgrounds regarding ANCA-related vasculitides in Japan and the United Kingdom, Japanese cases were older (72 vs. 61 years), predominantly subtype MPA, and had fewer cases of GPA. In addition, ANCA patterns revealed that 80% of cases in Japan were MPO-ANCA, while about 66% of cases in the United Kingdom were PR3-ANCA14). GPA usually progresses in the order of upper airway (ear), lung, and kidney. The condition without renal symptoms is referred to as localized GPA, and Japan has a higher incidence of this compared with other countries15). It is essential, therefore, that otolaryngologists who are familiar with GPA findings be involved early in the diagnostic process.
Pathology
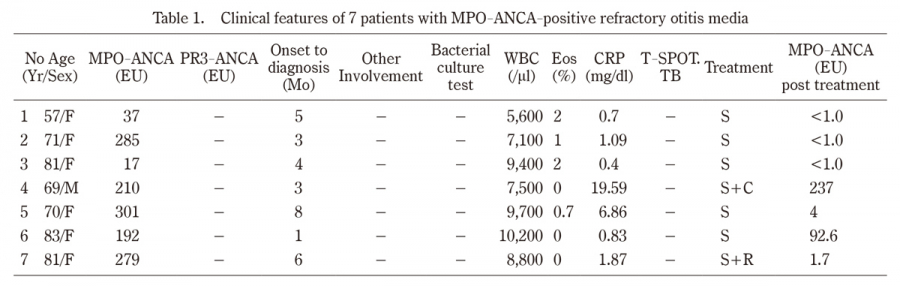
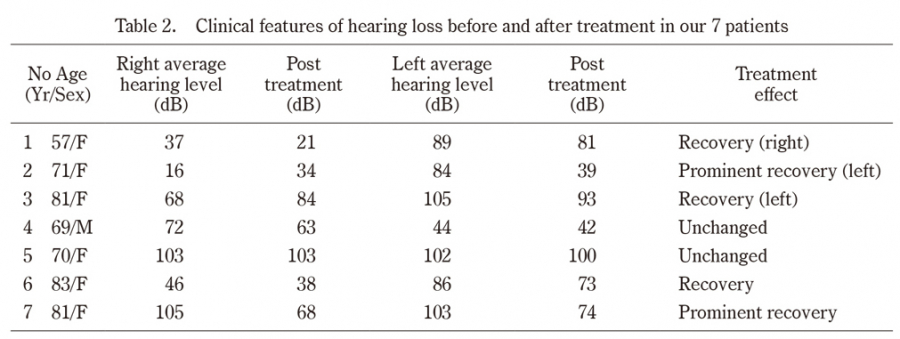
The specimens obtained from the mastoid cavity during mastoidectomy showed only nonspecific inflammatory cell infiltrates and necrotic tissue in Cases 1 and 2. We opted to perform mastoidectomy for confirmatory diagnosis in Cases 1 and 2 because it is difficult to determine whether AAV-induced intractable otitis media is associated with GPA, MPA, or EGPA at the initial visit. After all, no other AAV-related organ lesions are evident and neither case fulfilled the ordinary diagnostic criteria for systemic AAV, such as the JMHLW criteria and CHCC algorithm.
AAV sometimes develops with initial symptoms affecting the head and neck region16). It can be difficult to make a diagnosis from tissue biopsied from the affected region, including the upper airway, because the specimens obtained are often small, making it difficult to make a definitive pathological diagnosis in all cases17). In addition, taking biopsy specimens from the middle ear may result in facial palsy and worsening of ear symptoms associated with AAV18). Thus, clinicians can find it difficult, or even impossible, to identify the pathologic features of GPA.
It was reported that both vasculitis and necrosis were found in 23% of upper-airway biopsy specimens, vasculitis and granulomatous inflammation were present in 21%, while vasculitis, necrosis, and granulomatous inflammation were present in only 16%19,20). Diagnostically useful tissue in the upper airway was obtained, in decreasing order of frequency, from the paranasal sinuses, nose, and subglottic region. This order may reflect the quantity of tissue usually obtainable by biopsy. For example, previous studies reported that combined vasculitis and necrosis were found in 89% of samples taken from 82 open lung biopsies, whereas vasculitis was identified in only 4 specimens (7%) and granulomas were present in 3 of the 4 specimens of 59 transbronchial biopsies done in 48 patients19,21).
This difficulty in diagnosis often delays the initiation of treatment, occasionally allowing the disease to progress to an irreversible phase. Early diagnosis and treatment can prevent the need for dialysis and improve the prognosis of patients with AAV. CT and magnetic resonance imaging (MRI) are especially important when hypertrophic cranial pachymeningitis is suspected in cases of incurable headache, and cystography should be used for confirmatory diagnosis.
Etiology
A clinical feature of MPO-ANCA-associated hearing loss is that it is reversible if the hearing loss has not progressed to deafness. Significant recovery of hearing from sudden deafness due to ischemia of the cochlear microcirculation typically occurs within 1 to 2 months of onset. On the other hand, AAV patients have exhibited considerable reversibility in hearing levels with immunosuppressive therapy even after several months of hearing loss22). This reversibility indicates the hair cells are intact in the pretreatment state.
In GPA, the ear is frequently affected and many published studies describe clinical findings in this disease. In a clinical study of GPA, otologic involvement was commonly reported, with an incidence ranging from 19% to 47%23). McDonald et al.24) note three basic types of otologic involvement:(1) serous otitis media caused by nasopharyngeal ulceration and obstruction of the eustachian tube, (2) destruction of the middle ear and mastoid caused by actual involvement of the middle ear and mastoid cavity by GPA, and (3) sensorineural deficit caused by inflammation of the cochlear vessels. Common histologic findings are granulation tissue and bone absorption in the middle ear. Very few cases have inner ear lesions.
GPA can involve the middle ear and/or inner ear, causing conductive, sensorineural, or mixed hearing loss. An autoimmune inner ear disease is thought to cause sensorineural hearing loss in GPA. Okamura et al.25) reported a patient with GPA in whom sensorineural hearing loss was attributed to angiitis based on a positive antihuman neutrophil cytoplasm antibody test and improvement with steroid therapy. Ohtani et al.26) reported that the histopathology of GPA showed slightly atrophic stria vascularis and well-preserved spiral ganglion cells. Tympanic granulation tissue and inflammatory substances could also invade the inner ear through the round window. The histopathology of the temporal bone in GPA associated with complete deafness showed tympanic granulation tissue invasion of the round window niche and round window membrane, and projection into the tympanic duct.
Facial nerve palsy has also been reported as an initial symptom in GPA or as a presenting symptom associated with ear symptoms. Ohtani et al.26) also reported that the bony canal of the horizontal portion of the facial nerve is destroyed by granulation tissue that fills the tympanic cavity.
Treatment
Five of our 7 cases showed improvement with tapering steroid therapy and MPO-ANCA titer decreased in most cases. Although several clinical practice guidelines for the treatment of systemic AAV are available, therapies for AAV localized to the upper respiratory tract have not yet been standardized. Harabuchi et al. reported that treatment of ANCA-positive middle ear disease with glucocorticoids (GCs) and immunosuppressants could prevent disease relapse and progression of hearing loss more effectively than treatment with GCs alone. Based on the outcomes obtained with recent treatment guidelines, combined administration of both GCs and immunosuppressants is recommended as therapy for ANCA-positive middle ear disease27).
For AAV with lesions localized to the ear, prednisolone (0.3-1 mg/kg/day) and oral cyclophosphamide (25-75 mg/body/day) are recommended for remission induction therapy. For disease limited to the upper respiratory tract, the immunosuppressants recommended by recent clinical guidelines are monthly cyclophosphamide for pulse therapy (15 mg/kg/month) or oral azathioprine (0.5-1.5 mg/kg/day), and methotrexate (15-25 mg/week) every alternate week, as recommended by JMHLW. PSL dose reduction begins 1-2 weeks after local and hearing levels show remission, and the dose is tapered by 5-10 mg weekly up to 15-20 mg/day, which is maintained for at least 3 months2).
Prednisolone plus cyclophosphamide therapy is effective and remission can be achieved once in most patients with disease limited to the middle ear. However, long-term administration of cyclophosphamide can easily cause side effects such as infection, hematopoiesis, infertility, and bladder bleeding, and also carries a risk of carcinogenesis (mainly bladder cancer)28).
Harabuchi et al. studied 91 patients with GPA who were managed by an otolaryngologist in Japan. The upper respiratory tract alone was involved in 51 cases (56%). Although 21 of the 51 cases (41%) did not meet the Japanese diagnostic criteria initially, 13 of the 21 (62%) subsequently developed additional symptoms and signs during the observation period that did meet these criteria27,28).
Once initial regional AAV progresses systemically to organs, including the lung and kidney, and to the central nervous system in the absence of immunosuppressive therapy, AAV shows high mortality. It is important, therefore, that initial symptoms in the upper airway are considered with the inclusion of AAV in the differential diagnosis so that treatment can be started promptly. As infections are a trigger of AAV, this disease tends to localize in areas around the upper airway. Thus, otolaryngologists should be aware of the characteristic features of AAV-associated head and neck lesions and also that refractory otitis media is sometimes a presenting symptom of AAV. They should check for the presence of ANCA in such cases as soon as possible. Moreover, since AAV is a systemic disease, multidisciplinary input is required, involving nephrologists, rheumatologists, pulmonologists, and otolaryngologists, among others.
The combination of cyclophosphamide and GCs leads to remission in most patients with ANCA-associated vasculitides. However, even when patients receive maintenance treatment with immunosuppressive drugs, the relapse rate remains high. Rituximab may help to maintain remission. Yashiro-Furuta et al. reported that rituximab was effective in Japanese AAV patients and may be useful for prompt tapering of prednisolone, even in elderly patients who develop AAV29). Furthermore, Yoshida et al. reported that after starting immunosuppressive therapy, ANCA titers rapidly returned to the normal range and hearing levels improved, but that complete deafness could not be reversed22). In the present case series, hearing in Case 7 recovered from almost complete deafness after administration of rituximab. However, rituximab plus steroid combination therapy has been recently identified as a risk factor for hepatitis B virus reactivation in HBsAg-negative patients30). Therefore, we should consult internal medicine physicians from the early period of immunosuppressive therapy to avoid the risk of complications.