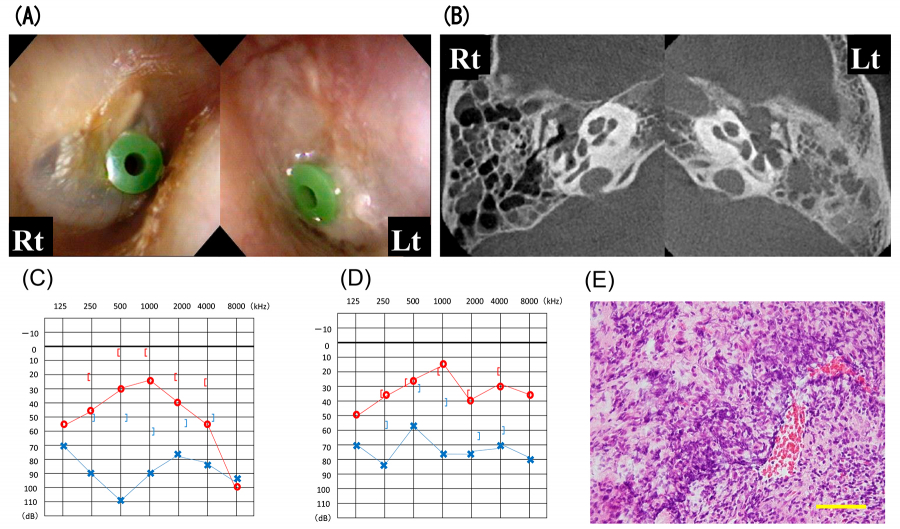
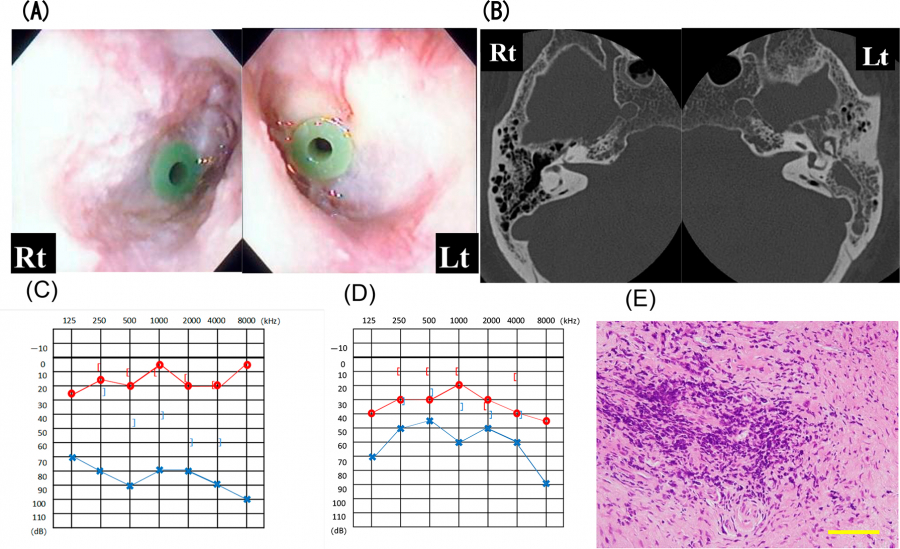
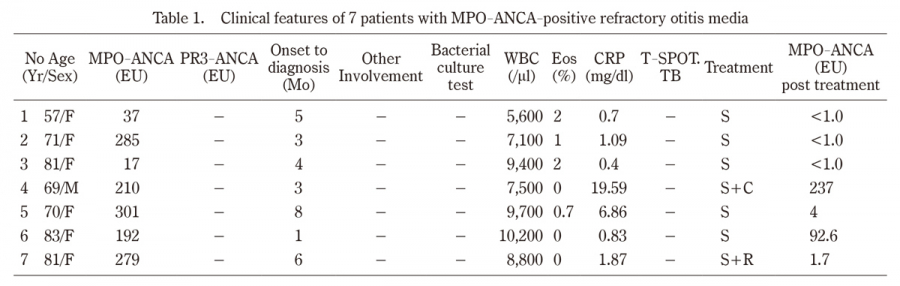
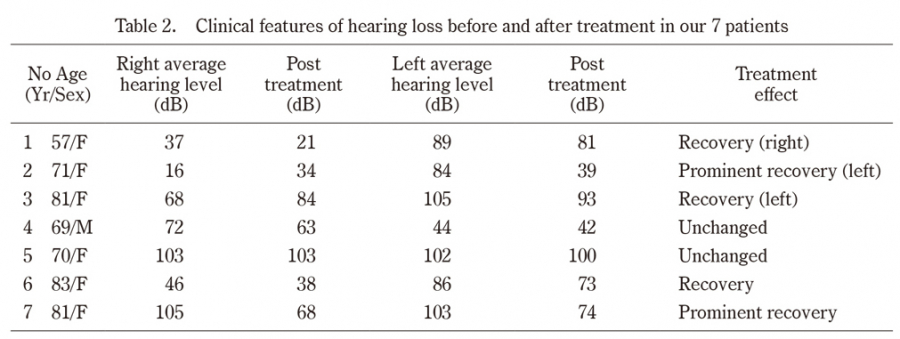
There are increasing reports of patients with refractory otitis media caused by anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV), especially myeloperoxidase (MPO)-ANCA-positive middle ear disease. However, making a definitive diagnosis can be difficult, which can adversely affect the outcome of treatment. We reviewed the diagnostic features of MPO-ANCA-positive middle ear disease and here discuss the difficulties of timely diagnosis and treatment. Seven cases were eligible (6 women, 1 man;aged 57-83 years), and all were MPO-ANCA positive and proteinase 3 (PR3)-ANCA negative. The patients were referred to our institution for management of intractable otitis media (2/7), progressive hearing loss (7/7) with facial palsy (1/7), and/or a high MPO-ANCA titer (5/7). All patients underwent tapering steroid therapy and their MPO-ANCA titer was monitored. Refractory MPO-ANCA-positive otitis media was noted:5 of 7 cases showed improvement with tapering steroid therapy but cure was not achieved in the remaining 2 cases. This study demonstrates the difficulties in the diagnosis and treatment of localized AAV. Early diagnosis and treatment can improve the prognosis of patients with AAV but global diagnostic criteria for ear disease have not been established. Additional cases should be prospectively examined to establish a treatment for MPO-ANCA-positive middle ear disease.
Abstract/References
Seven cases illustrating difficulties in the treatment of MPO-ANCA-positive refractory otitis media
Koshi Otsuki, Mitsuyoshi Imaizumi, Shigeyuki Murono
-
Koshi Otsuki
Otsuki ENT Clinic
-
Mitsuyoshi Imaizumi
Department of Otolaryngology Fukushima Medical University
-
Shigeyuki Murono
Department of Otolaryngology Fukushima Medical University
Abstract
References
1. Kallenberg CG, Heeringa P, Stegeman CA, et al. Mechanism of Disease:pathogenesis and treatment of ANCA-associated vasculitides. Nat Clin Pract Rheumatol, 2:661-670, 2006.
3. Jennette JC. Overview of the 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Clin Exp Nephrol, 17(5):603-606, 2013.
5. Balow JE. Renal vasculitis. Curr Opin Nephrol Hypertens, 2:231-7, 1993.
6. Kallenberg CG. Pathogenesis of ANCA-associated vasculitides. Ann Rheum Dis, 70:i59-63, 2011.
8. Savige J, Gillis D, Benson E, et al. International Consensus Statement on testing and reporting of antineutrophil cytoplasmic antibodies (ANCA). Am J Clin Pathol, 111:507-513, 1999.
15. Hashimoto H. Study on clinical epidemiology investigation between Japan and Europe of the ANCA-related vasculitis and diagnostic agent and therapy development 2007 (in Japanese).
20. Devaney KO, Travis WD, Hoffman GS, et al. Interpretation of head and neck biopsies in Wegener’s granulomatosis. A pathologic study of 126 biopsies in 70 patients. Am J Surg Pathol, 14: 555-564, 1990.
21. Travis WD, Hoffman GS, Leavitt RY, et al. Surgical pathology of the lung in Wegener’s granulomatosis. Review of 87 open lung biopsies from 67 patients. Am J Surg Pathol, 15:315-333, 1991.
23. McDonald TJ, DeRemee RA. Wegener’s granulomatosis. Laryngoscope, 93:220-231, 1983.
26. Ohtani I, Baba Y, Suzuki C, et al. Temporal bone pathology in Wegener’s granulomatosis. Fukushima J Med Sci, 46:31-39, 2000.
27. Harabuchi Y, Kishibe K, Tateyama K, et al. Clinical features and treatment outcomes of otitis media with antineutronphil cytoplasmic antibody (ANCA)-associated vasculitis (OMAAV):a retrospective analysis of 235 patients from a nationwide survey in Japan. Mod Rheumatol, 27(1):87-94, 2017.
29. Yashiro-Furuya, et al. Outcome of rituximab treatment in Japanese patients with ANCA-associated vasculitis in daily clinical practice:A two-centre study in Fukushima, Japan. Mod Rheumatol, 33(2):352-359, 2023.
Figures