We explored the use of CAD/CAM technology with small-scale 3D printers for its potential impact on the production of prosthetic orthoses. We conducted fit evaluations and examined the suitability of this approach for small-and medium-sized prosthetic orthosis companies.
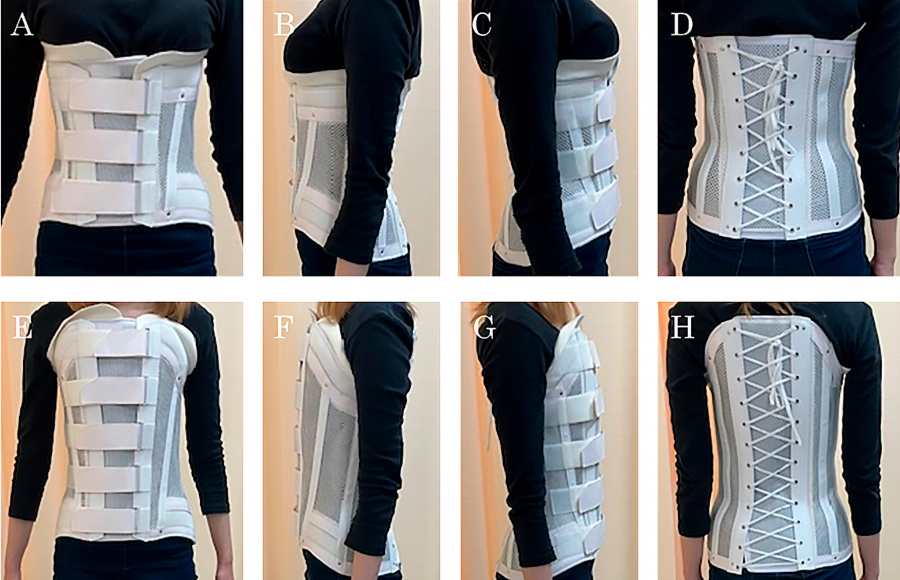
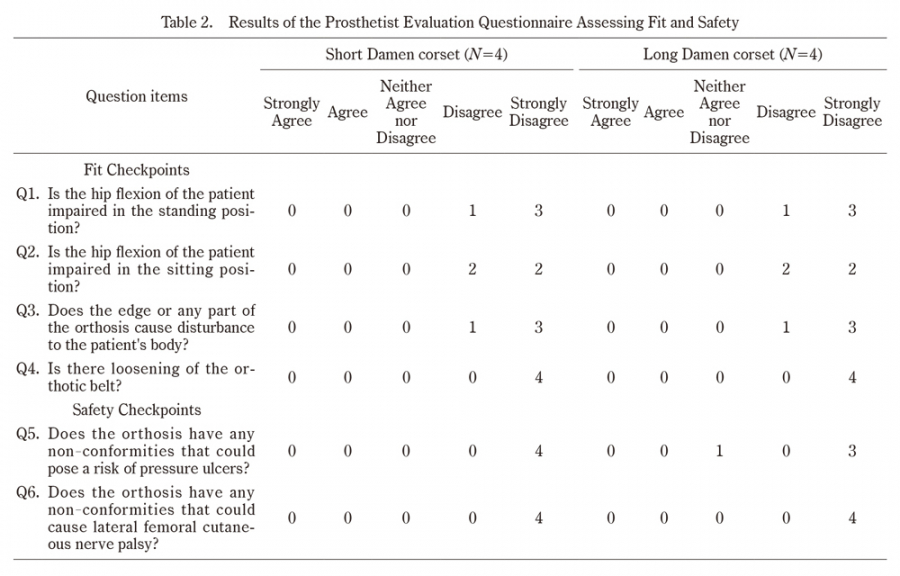
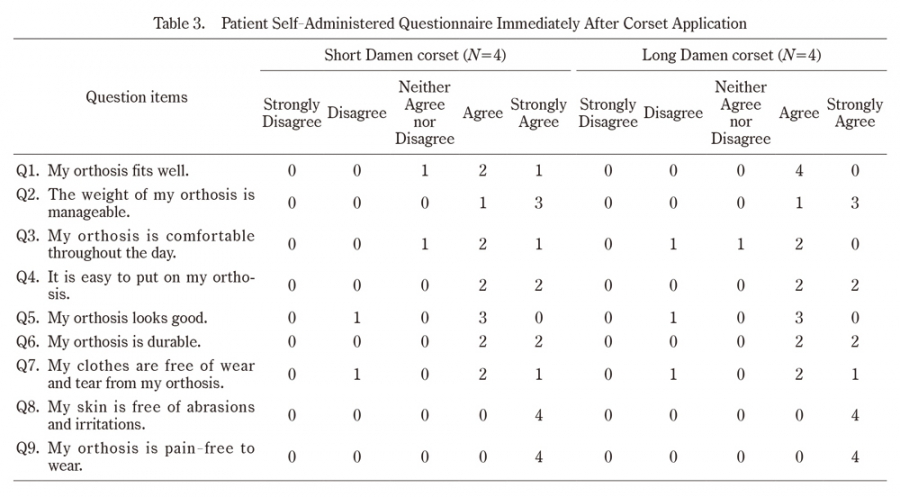
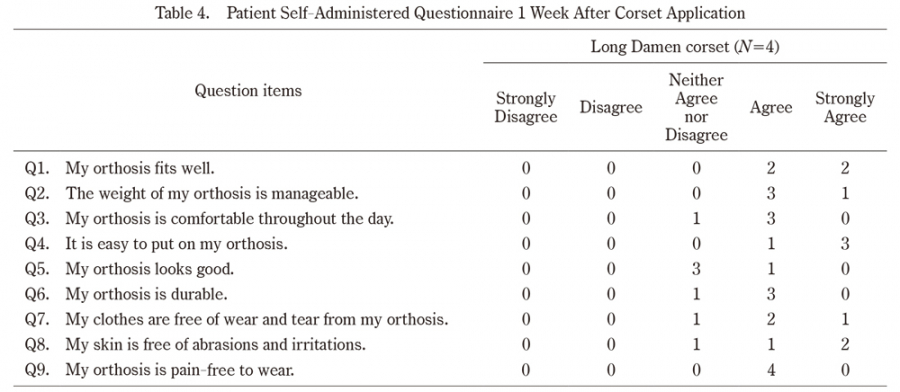
Fit evaluation by the prosthetist confirmed the validity of the proposed method, demonstrating that the CAD/CAM approach using a small 3D printer and CT data can produce orthoses anatomically aligned with the patient’s body. Subjective feedback was favorable, supporting the comfort and functionality of CAD/CAM-based orthoses, and no significant deterioration in the wearing experience was observed after 1 week of continuous wear. One participant was dissatisfied with the comfort of the orthosis during the day immediately after wearing it, although it was well received by all at the 1-week evaluation. Problems related to esthetic preferences and clothing wear probably stem from the quality of the orthosis itself rather than the method. In summary, both prosthetists and patients reacted positively to the corsets made using our method, highlighting the potential of 3D printing in prosthetic manufacturing.
Pain Reduction
A primary advantage of our proposed method is pain reduction during casting, which is particularly crucial in patients with vertebral fractures. Traditional plaster casting causes discomfort, hindering ideal posture and extended molding periods. Traditional casting processes often cause discomfort and pain in patients. However, CAD/CAM allows digital data collection, particularly CT data, effectively avoiding casting-related pain. This approach enables patients to receive orthoses, facilitating early rehabilitation1,12).
Fit and Comfort Provided by the Orthosis
We chose soft orthotics as the end product of the CAD/CAM process. Spinal orthoses can be divided into two categories:rigid (including semi-rigid) or soft orthoses13). Properly fitted orthosis improves patient comfort and compliance and increases the likelihood of successful treatment13). Orthotic fit cannot be ignored, and differences in body shape caused by differences between the supine and upright positions14)are hypothesized to have a negative impact on orthotic fit. A soft orthosis is more flexible and adaptable to changes in body shape. Rigid orthoses provide higher spinal stability than soft orthoses15). However, in our main target group (patients with vertebral fractures), the clinical difference in treatment outcomes between rigid and soft orthoses was minimal16),which is why we produced a soft orthosis using our method.
Manufacturing Process Improvement
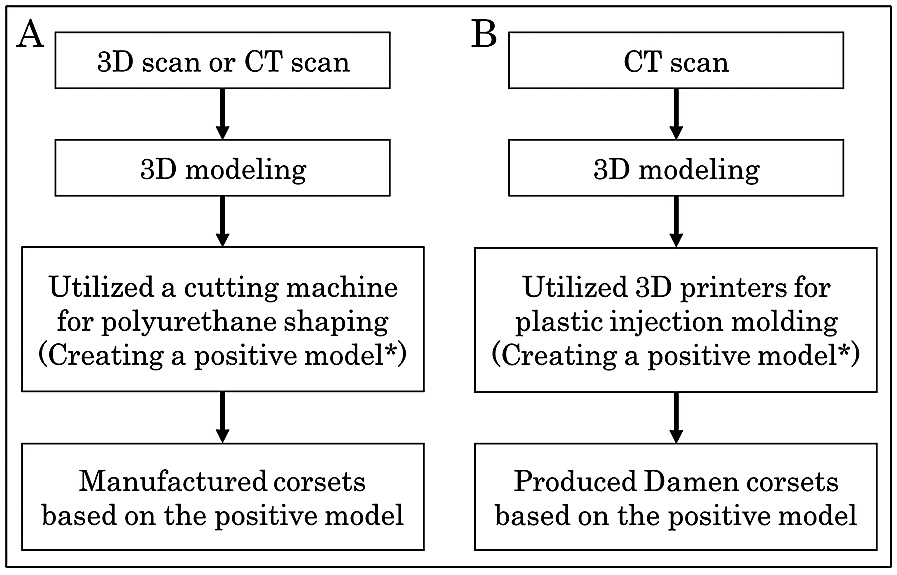
CAD/CAM has streamlined the process from orthotic design to production. Design data can be directly transmitted to computer-controlled manufacturing equipment, enabling rapid production. In many countries, orthosis manufacturing using CAD/CAM is widely practiced, resulting in high operational efficiency3,4,17). Further, substantial cost reductions and increased efficiency have been reported compared with traditional methods. In some regions, traditional casting methods remain mainstream, and CAD/CAM-based molding methods have not gained widespread adoption in orthosis manufacturing. In regions and facilities where it is feasible, the adoption of CAD/CAM-based techniques should be considered.
Reduction of Initial Implementation Costs for CAD/CAM Integration
Our approach reduces the initial costs, especially for facilities introducing CAD/CAM technology. Traditional CAD/CAM manufacturing methods require the purchase of an expensive carving machine, which incurs a substantial initial investment. In a price comparison with the manufacturing equipment used in a previous report18), the initial cost required for a carving machine was $200,000, versus $10,000 for 3D printers. The small 3D printers that we used cost approximately $1,000 each. Employing our method with approximately 10 of these small 3D printers would result in a total cost of approximately $10,000, which is similar to that described in previous reports.
CT Radiation Exposure, Cost, and Benefits of Our System
The use of CT imaging in our corset manufacturing system is essential, although some concerns exist, especially regarding potential radiation exposure from CT;this is a significant consideration for both patients and physicians.
However, societal acceptance exists related to enhancing the quality of orthopedic treatments by leveraging CT data. Procedures such as joint replacements and spinal surgeries already utilize CT data for navigation and robotic-assisted surgeries. In our system, the use of CT imaging allows us to supply corsets more rapidly compared with conventional methods, which is beneficial in regions where the time to provide an orthotic is delayed. This advantage may outweigh the associated costs and shortcomings of CT.
Clinical Indications for Our Product
Our system produces the Damen corset as the final product, which we believe can be applied to conditions previously treated with Damen corsets. In particular, our product is suitable for patients with lumbar or thoracolumbar vertebral fractures, especially patients who have difficulty maintaining an upright position or desire early corset supply. It is important to note that our product may not be suitable in all cases. Specifically, it is not appropriate for situations with unstable vertebral fractures, such as burst fractures. Clinicians must properly assess the patient’s condition to determine whether our product is an appropriate.
Influence of Our Method on Corset Provision in Japan
Our product is anticipated to alleviate regional variations in orthotic supply across Japan, thereby enhancing the overall quality of healthcare. The provision of a corset in Japan typically involves three hospital visits for patients. The first visit entails receiving a diagnosis of vertebral fractures after an injury and obtaining a prescription for a corset from a physician. The second visit involves a prosthetist creating a mold (casting) based on the patient’s body shape, resulting in a significant initial waiting period. The third visit occurs after the corset is manufactured and the patient returns to receive and wear the corset. In medically underserved areas in Japan, where prosthetists are only available once a week or less, patients often have to wait for approximately 2 weeks or more.
We aim to streamline this process by introducing CAD-based orthopedic device manufacturing methods, which greatly reduce waiting times. Patients will no longer need to wait for mold creation after receiving a prescription because orthopedic devices created using CT data will be provided during the first follow-up visit. By implementing this method, the corset supply period can be reduced to approximately 1 week in medically underserved areas, facilitating early treatment and rehabilitation for patients.
However, despite the evident benefits of CAD/CAM corsets, the lack of insurance coverage in Japan has hindered their widespread adoption. Japan’s National Health Insurance program has a mandate to enroll all residents. This system helps to alleviate the financial burden of healthcare costs in Japan and ensures widespread access to medical services. Within this framework, the Japanese healthcare insurance system manages coverage of specific medical devices and treatments. To achieve insurance coverage for CAD/CAM orthopedic devices in Japan, continued research and dissemination of information on their utility, safety, and cost-effectiveness is crucial.
Limitations
This study has some limitations. Evaluations were conducted in patients without spinal disorders, necessitating further research to assess the long-term durability and effectiveness in patients with specific conditions.
We applied the OPUS-CSD-J to assess the fit and comfort of the patient’s orthosis. According to a previous study11), the OPUS-CSD-J is considered unreliable when used to assess orthotics, as the Cronbach’s alpha coefficient was 0.63, which is less than 0.7. However, we consider its value to be moderate and, given that the questions comprising the OPUS-CSD-J scale consist of items that represent the participants’ subjective conformity and comfort, the actual use of this scale is acceptable with the understanding of this limitation.
Additionally, comparative studies of traditional versus CAD-CAM corsets for various outcomes (pain, physical function, and medical-economic indicators) are needed. While this study focused on Damen corset orthosis manufacturing, expanding this approach to other types of prosthetic orthoses is subject to future research.
Finally, it should be noted that applying our system directly in some regions may pose challenges, which may be a limitation of our system. We have developed a system to reduce regional disparities in the supply of corsets. However, it is anticipated that in areas with limited medical resources, there may be clinics or hospitals where CT scans cannot always be conducted in a timely manner. Going forward, efforts will be needed to explore solutions to address this issue.
Conclusion
The CAD/CAM-based prosthetic orthosis manufacturing approach using small-scale 3D printers is a promising solution for remote orthosis production. This method enhances patient care and accessibility while maintaining cost-effectiveness, making it an attractive option for prosthetic orthosis companies. Further research and refinement of this innovative approach are expected to expand its applicability.