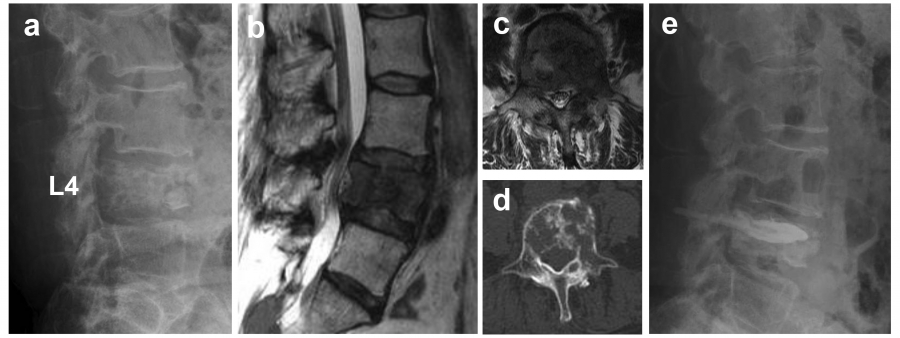
Spinal cord tumors are broadly classified into intramedullary, intradural, extramedullary, epidural, or spinal dumbbell tumors (SDT). SDT extend into or out of the spinal canal and have an hourglass-like appearance.
SDT, including schwannomas, are frequently benign tumors. However, PMST, such as malignant peripheral nerve sheath tumors (MPNST), can occur as malignant SDT (MSDT). Although challenging, MSDT can be cured with appropriate treatment at the localized stage. However, most MSDT proliferate rapidly and often cause neurological damage as they spread in the spinal canal.
Therefore, a prompt and accurate diagnosis is necessary. In fact, in many cases, histological analysis is required for a correct diagnosis, as there are many histologic types of MSDT. A biopsy is necessary for a definitive diagnosis; however, if the tumor is located in close proximity to adjacent vital organs such as blood vessels or the intestinal tract, it may require highly invasive maneuvers.
In contrast, benign SDT (BSDT) such as schwannomas have an indolent course, and resection can be avoided in such cases, which often discourages invasive biopsy. However, no method has been established to differentiate between BSDT and MSDT based on imaging. Therefore, we compared the imaging features of MSDT with those of BSDT and developed a simple scoring method to determine the benign or malignant status before surgery.
We included 59 patients with histologically confirmed SDT. The histological diagnoses and number of cases are shown in Table 1. A dumbbell scoring system (DSS) was developed and statistically analyzed by extracting the features of computed tomography (CT) and MRI images. The factors included in the DSS were: tumor diameter >5 cm (two points), indistinct borders (2 points), lobular morphology (1 point), and bone destruction (1 point), which were significantly more common in malignant tumors (Table 2). In each case, the scores were summed and the DSS score was calculated; the median DSS score was 0 for benign tumors and 5.5 for malignant tumors. Using 3 points as the threshold, differentiation between benign and malignant tumors was achieved with a sensitivity of 90% and a specificity of 84.6%. This indicated a high probability of differentiation between BSDT and MSDT1).
If malignancy is suspected by scoring, a definitive diagnosis can be made using CT-guided biopsy, which enables appropriate treatment planning, including consideration of additional preoperative chemotherapy and selection of a reliable surgical method to secure the resection margin. If the score is below the cutoff value, careful follow-up is also an option. However, the present analysis was a retrospective study with a limited number of cases, and future multicenter prospective validation is necessary to generalize the scoring system.
A new modality recently introduced is PET-MRI, which has begun clinical applications2). PET-MRI has several advantages over PET-CT. In pediatric imaging, multiple CT scans performed over a long period of time are known to increase the risk of developing secondary cancers3). PET-MRI, on the other hand, requires less radiation exposure than PET-CT, reportedly reducing the cumulative dose by 50-70% during follow-up for pediatric lymphatic tumors4).
In addition, MRI provides greater contrast, owing to differences in soft tissue organization, allowing for an accurate assessment of the extent of tumor extension. With this advantage, a report on limb-onset osteosarcoma found that the maximum standardized uptake values inside the tumor after preoperative chemotherapy were significantly correlated with the efficacy of chemotherapy5). A similar analysis was performed using PET/CT, but the results were not comparable with those obtained using PET-MRI6).
Furthermore, PET-MRI can identify tumor extension in the spinal canal and surrounding soft tissues of the paraspinal region, especially in the vicinity of neural tissue, and is useful in determining the extent of resection, radiation, and other treatment strategies. Thus, it may be effective for the diagnosis and treatment of PMST. However, studies on the usefulness of PET-MRI in PMST are scarce, and further validation is required.
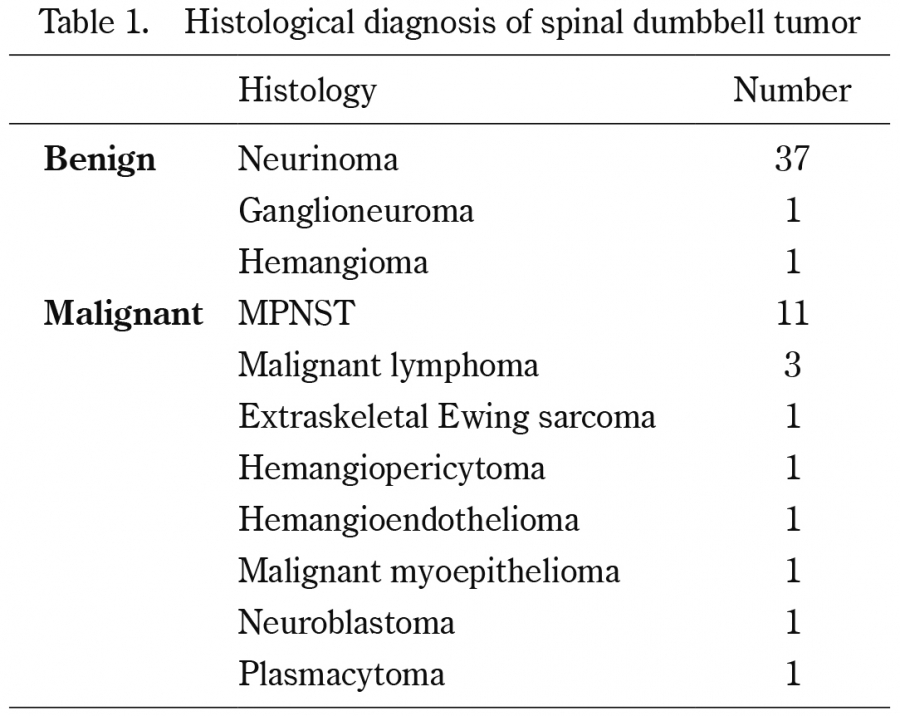
Table 1.
Histological diagnosis of spinal dumbbell tumor
MPNST: Malignant peripheral nerve sheath tumor
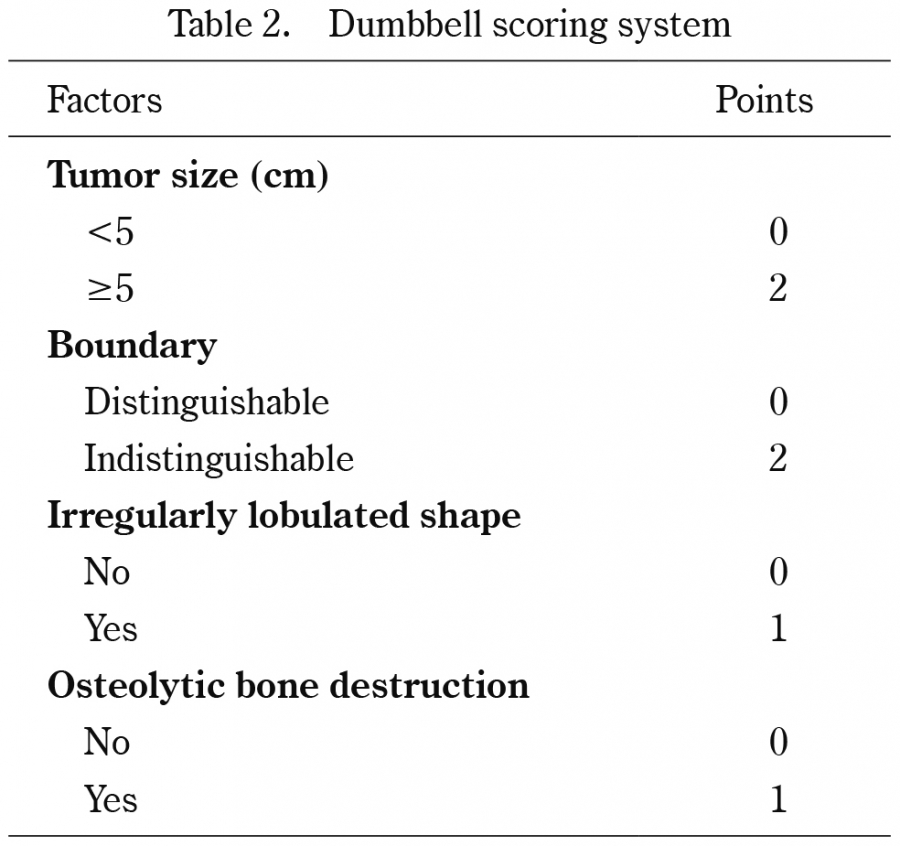
Table 2.
Dumbbell scoring system
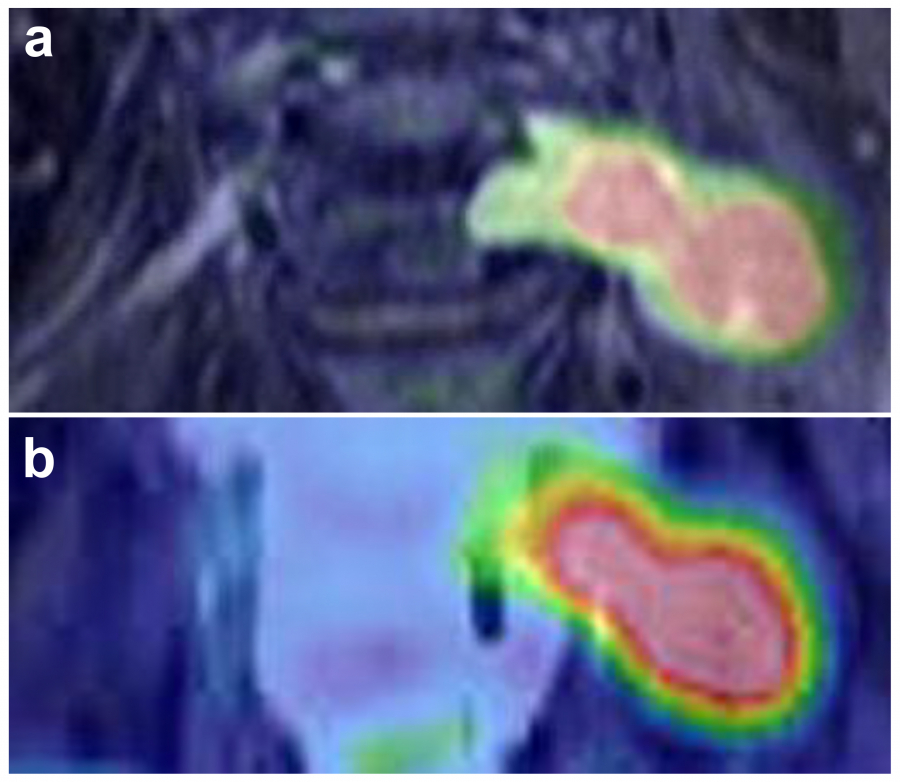
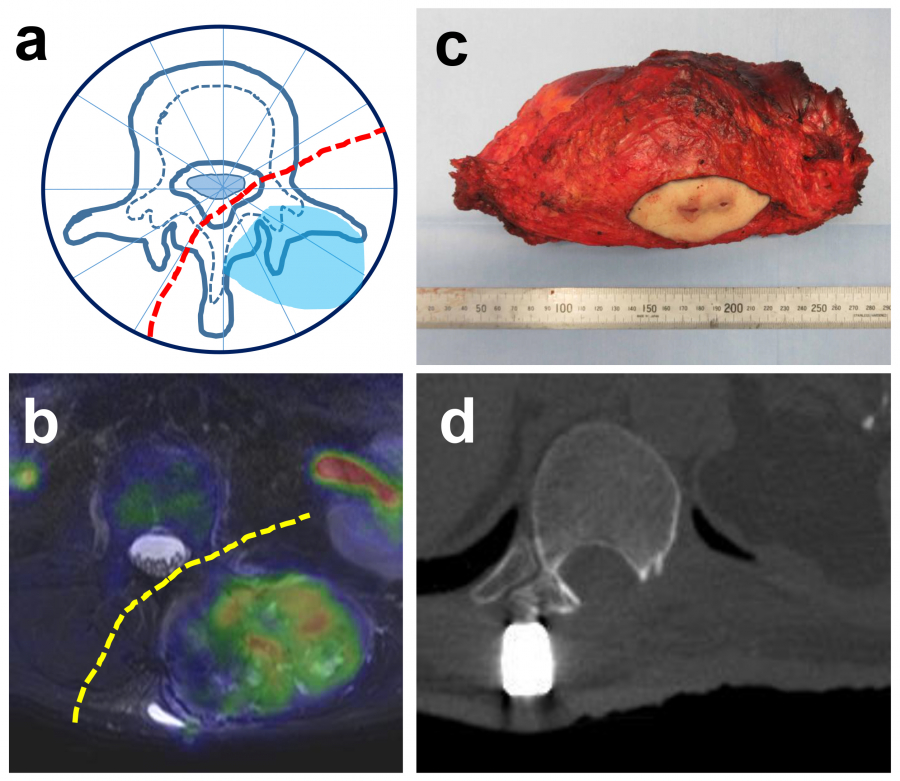
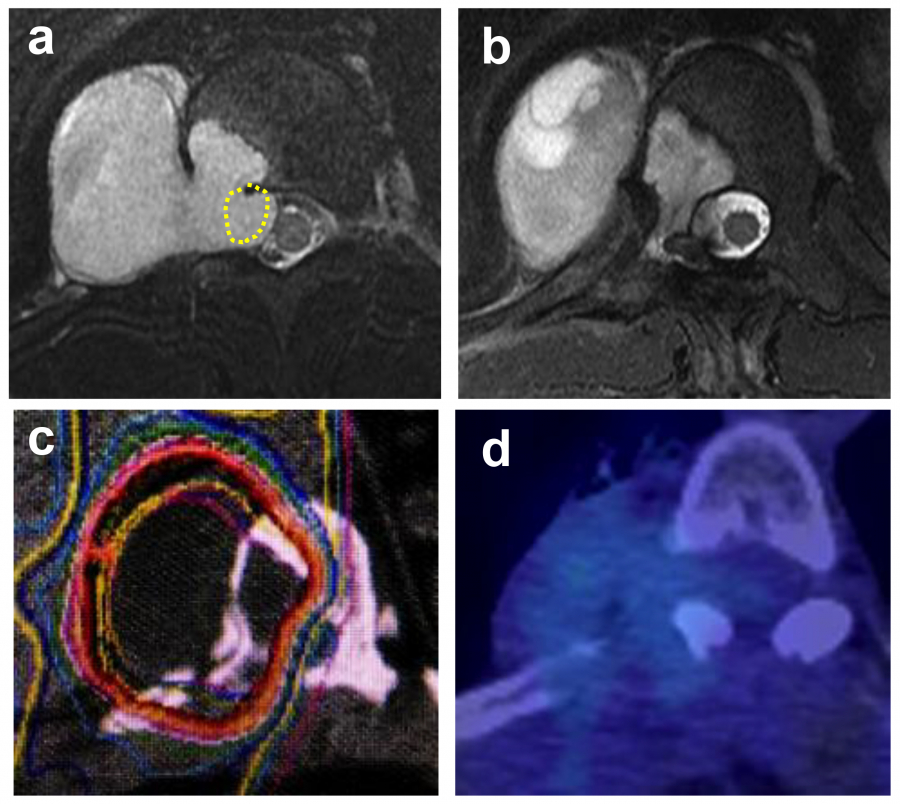
Fig. 1.
Positron emission tomography and magnetic resonance imaging (PET-MRI). (a) PET-MRI fusion image, (b) PET-computed tomography (CT) fusion image. Compared to PET-CT fusion images, PET-MRI fusion images demonstrate superior spatial resolution, clearly depicting tumors and surrounding tissues.