

A systematic review with meta-analyses was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, and was registered in the International Prospective Register of Systematic Reviews (registration number CRD42023398206)
The content of research paper
Relationship between quality of life before treatment and survival in patients with hematological malignancies: A meta-analysis
Keiichi Osaki, Shinichiro Morishita, Jiro Nakano, Junichiro Inoue, Taro Okayama, Katsuyoshi Suzuki, Takashi Tanaka, Takuya Fukushima
Author information
-
Keiichi Osaki
Department of Rehabilitation, Panasonic Health Insurance Organization, Matsushita Memorial Hospital
-
Shinichiro Morishita
Department of Physical Therapy, School of Health Sciences, Fukushima Medical University School of Health Science
-
Jiro Nakano
Faculty of Rehabilitation, Kansai Medical University
-
Junichiro Inoue
Division of Rehabilitation Medicine, Kobe University Hospital International Clinical Cancer Research Center
-
Taro Okayama
Division of Rehabilitation Medicine, Shizuoka Cancer Center
-
Katsuyoshi Suzuki
Division of Rehabilitation Medicine, Shizuoka Cancer Center
-
Takashi Tanaka
Department of Rehabilitation, Hyogo Medical University Hospital
-
Takuya Fukushima
Faculty of Rehabilitation, Kansai Medical University
Trial registration
Statements and Declarations
The authors have no conflicts of interest to declare.
Introduction
In recent years, advances in therapy and the development of supportive care have expanded the range of treatment options for cancer patients, resulting in improved survival rates. However, alongside therapeutic advancements, there is a growing challenge of treatment-related adverse events. Therapies for hematological malignancies continue to evolve with the development of new drugs, often involving long-term treatment courses. The complexity of the pathophysiology and treatment modalities of these diseases may profoundly impact the quality of life (QoL) and overall survival (OS) of patients.
Adverse events associated with cancer treatment, such as fatigue and anorexia, are common and contribute to a decline in physical function and activity levels, exacerbating the impact of treatment1-4). There exists a close relationship between physical function, physical activity, and QoL, with reports across various cancer types indicating a decline in QoL associated with decreases in grip strength and lower limb function5-7). Moreover, low levels of physical activity have been linked to decreased QoL in cancer patients8-10). Additionally, factors affecting mental well-being, such as anxiety and depression, also influence QoL11,12). Cancer patients often experience psychological stress related to treatment-related anxieties, fatigue, and other physical symptoms, further complicating QoL considerations. Therefore, addressing both physical and psychological aspects is essential in evaluating QoL in cancer patients. Furthermore, social factors such as personal economic situation and education have been reported to be associated with QoL in chemotherapy-treated cancer patients, emphasizing the importance of patient backgrounds13-15).
Recently, it has become clear that QoL also affects OS, further increasing the importance of QoL during cancer treatment. Zang et al.16) reported in a meta-analysis that baseline health-related QoL defined by physical function or the global QoL scale of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C30 (EORTC QLQ-C30) predicts OS in digestive cancer patients. Moreover, their study also found that reduced global QoL, physical functioning, social functioning, and role functioning scales were significantly associated with decreased OS. Studies investigating QoL and OS in various cancer types and cancer survivors are ongoing, with QoL emerging as a significant predictor of OS17-21). However, there are conflicting reports, suggesting that the relationship between QoL and OS remains unclear in certain cancer stages22). Consequently, many aspects of the relationship between QoL and OS have yet to be elucidated.
Notably, research on QoL and OS in the field of hematological malignancies is limited. Among the reviews reported to date that encompassed various cancer types, very few have included hematological malignancies23,24). It is not clear which function parameters of QoL are involved in OS in patients with hematological malignancies, and there have been no studies stratified by treatment content. Factors related to QoL may vary among hematological malignancy patients, depending on the content and intensity of treatments such as hematopoietic stem cell transplantation (HSCT) and chemotherapy. Despite the possibility that there may be differences in the effect of each function parameter of QoL on OS, there are currently no reports on this point. Understanding the relationship between QoL and OS at the pretreatment stage would further emphasize the importance of intervention. Depending on the results, it may also support interventions by healthcare providers to maintain patients’ QoL. Therefore, in this study, we aimed to investigate whether QoL affects OS, focusing specifically on hematological malignancy patients undergoing HSCT and chemotherapy, stratifying and analyzing them through meta-analysis.
Methods
A systematic review with meta-analyses was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, and was registered in the International Prospective Register of Systematic Reviews (registration number CRD42023398206)25,26).
Data searches and sources
Cumulative Index to Nursing and Allied Health Literature (CINAHL), PubMed/MEDLINE, and Scopus databases from inception to December 2022 were searched based on QoL, EORTC QLQ-C3027), Medical Outcomes Study Short-Form 36-Item Health Survey28), Functional Assessment of Cancer Therapy-General (FACT-G)29), as well as cancer, neoplasms, tumors, sarcomas, hematological malignancies, lymphomas, carcinosarcomas, leukemia, mortality, survival, relapses, and recurrences.
Study eligibility criteria and study selection
The study eligibility criteria were as follows:1) observational studies; 2) original human studies published in English; 3) patients with hematological malignancies in the pretreatment setting; 4) patients treated with chemotherapy or HSCT; and 5) studies on the relationship between QoL and mortality. Studies that examined the relationship between symptoms and mortality were excluded. After duplicates were removed, eight reviewers (TF, JN, SM, JI, TO, TT, KS, and KO) independently assessed study eligibility by reviewing the titles and abstracts of all potential citations according to the eligibility criteria. Full-text articles were retrieved for review if there was evidence of meeting the eligibility criteria or if there was insufficient information in the abstract or title. Final inclusion of eligible observational studies was determined in consensus meetings attended by all authors.
Data extraction
Two reviewers (TF and JN) were responsible for data extraction. The following data were extracted from each included study:1) last name of the first author; 2) year of publication; 3) study location; 4) treatment (chemotherapy or HSCT); 5) number of patients; 6) sex; 7) age; 8) QoL assessments; 9) follow-up time; 10) covariates adjusted for in multivariate analysis; 11) number of deaths; and 12) risk estimates for mortality (hazard ratio [HR] and 95% confidence interval [CI]). When multiple models of multivariate analyses were reported, we used the results from the model with the most complete adjustment for potential confounders.
Quality assessment
The Newcastle-Ottawa Scale was used to assess the quality of studies, including their risk of bias30). There are eight domains within this tool: representativeness of the exposed cohort; selection of the non-exposed cohort; ascertainment of exposure; demonstration that the outcome of interest was not present at the beginning of the study; comparability of cohorts based on design or analysis; assessment of outcomes; whether the follow-up period was sufficient for outcomes to occur; and whether cohort follow-up was adequate. The items were scored by two trained reviewers in accordance with the criteria. Consensus meetings attended by all authors were used to resolve potential disagreements.
Data analysis
Risk estimates for total mortality associated with global QOL and its subscales (physical, emotional, role, social) were analyzed. In an additional analysis, we examined the associations between global and subscales of QoL and total mortality by treatment (chemotherapy and HSCT). We used adjusted HRs and 95% CIs in the multivariate analysis as a measure of effect size for all studies. The univariate HR was used only if reported, but not the multivariate HR. For inverse variance-weighted means, the natural logarithmic HR was used, and the standard error was calculated using a random effects model. We also assessed heterogeneity using the I2 statistic. All statistical analyses were performed with Review Manager version 5.1 (RevMan; The Cochrane Collaboration, London, UK).
Results
The literature search yielded 119,061 articles, which was reduced to 2,483 articles after excluding duplicates and patients without hematological malignancies. Based on the screening of titles and abstracts, seven articles were deemed eligible and underwent full-text review. After review, one article was excluded because it was not a pretreatment setting. Finally, six articles were identified and determined to be suitable for meta-analysis (Fig. 1).
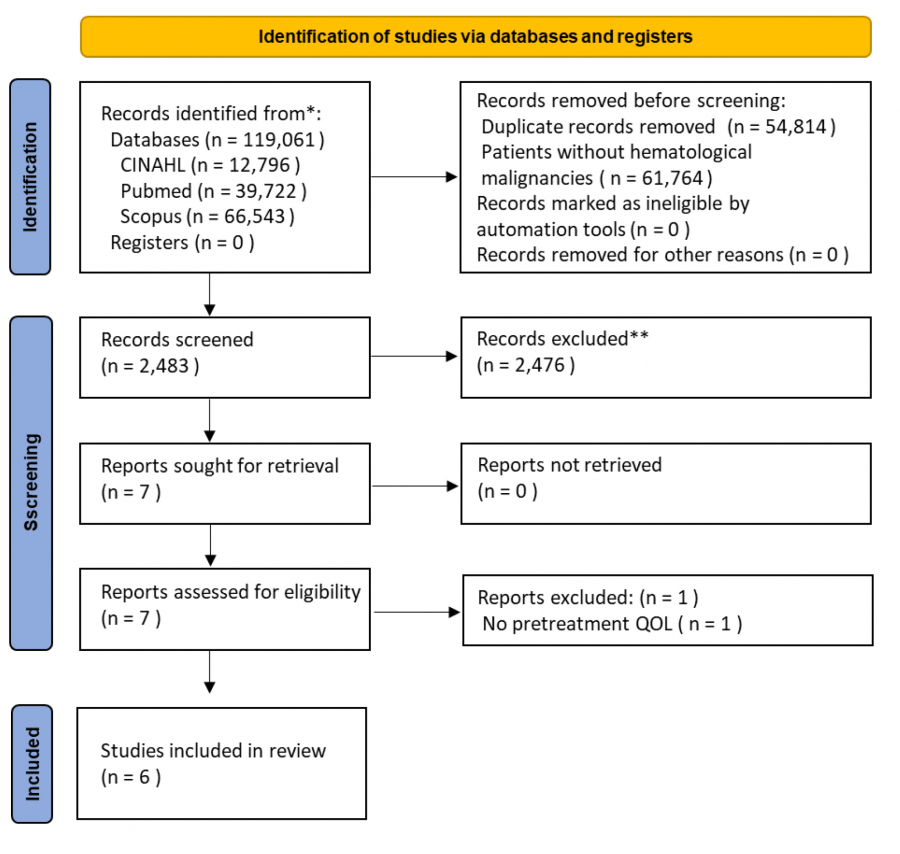
Fig. 1.
Study flow diagram of the selection process
Study characteristics
The characteristics of the included studies are summarized in Table 1. This meta-analysis included a total of 2,202 patients from studies conducted in different countries. The mean age was 46–51 years, and 27–48% were female. There were two articles on HSCT31,32) and four articles on chemotherapy33-36). QoL was assessed using the EORTC QLQ-C3033-36), FACT-G31), and EuroQol 5 Dimensions32). Both of the HSCT studies that were employed involved patients with a variety of hematological malignancies. All four studies on chemotherapy included lymphoma patients only.
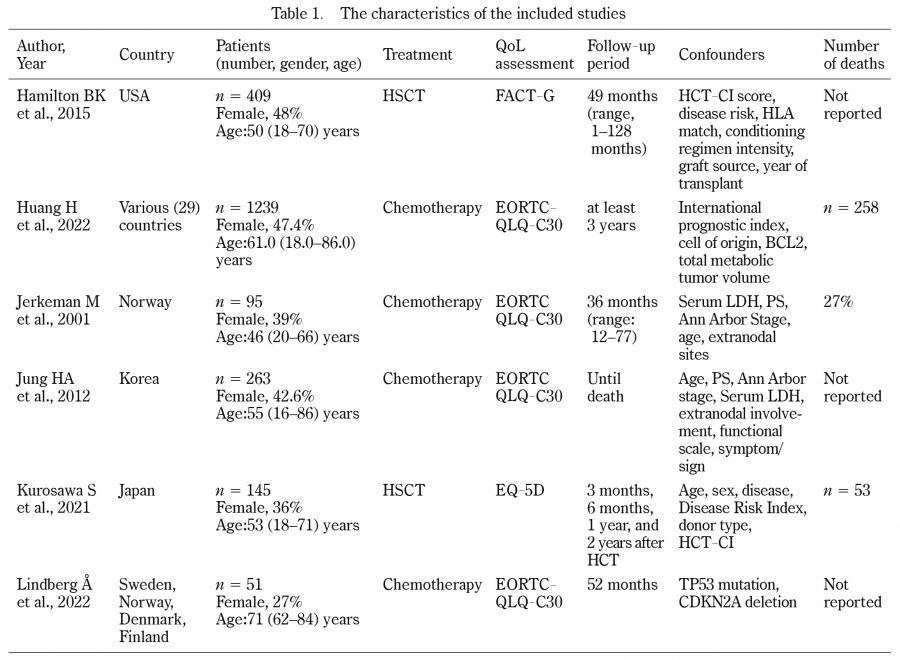
Table 1.
The characteristics of the included studies
EORTC QLQ-C30, The European Organization for Research and Treatment of Cancer QLQ-C30; EQ-5D, EuroQol 5 Dimensions; HCT-CI, Hematopoietic Cell Transplantation-specific Comorbidity Index; HLA, human leukocyte antigen; HSCT, hematopoietic stem cell transplantation; LDH, lactate dehydrogenase; PS, performance status; USA, United States of America.
Risk of bias assessment
Risk of bias was assessed using the Newcastle-Ottawa Scale. Of the included studies, four were considered to be of high impact (8–9 points) and two were considered to be of moderate impact (6–7 points) (Table 2).
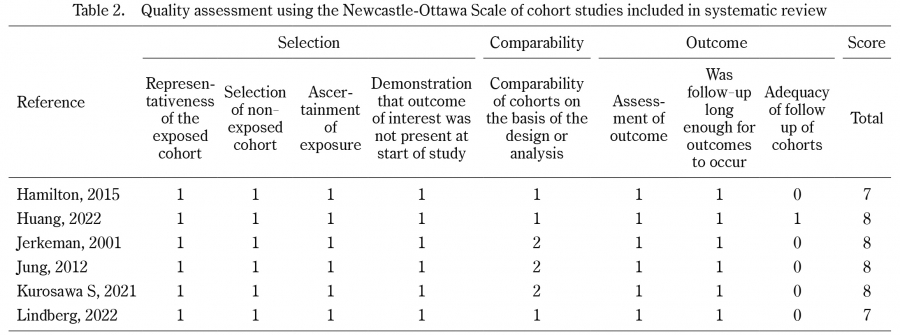
Table 2.
Quality assessment using the Newcastle-Ottawa Scale of cohort studies included in systematic review
Association between global QoL and mortality risk
A random-effects meta-analysis included a total of six studies. A forest plot of inverse HR and 95% CI was used to estimate the association between global QoL and mortality risk. Overall, global QoL was significantly associated with mortality risk (HR:1.04, 95% CI:1.01–1.08, p = 0.01). A subgroup analysis by treatment showed borderline significance between global QoL and mortality risk in both HSCT (HR:1.05, 95% CI:1.00–1.11, p = 0.05, I2 = 0%) and chemotherapy (HR:1.04, 95% CI:1.00–1.09, p = 0.05, I2 = 74%). There were no significant differences between the subgroups (p = 0.73) (Fig. 2).
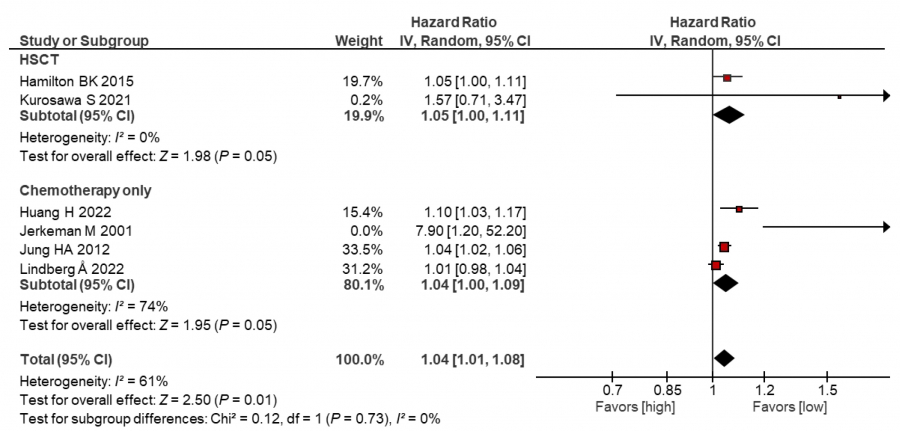
Fig. 2.
Meta-analysis of the association between global QoL and mortality risk in patients with hematological malignancies
Association between physical QoL and mortality risk
Four studies were included in a random-effects meta-analysis. Overall, there was a significant association between physical QoL and mortality risk (HR:1.06, 95% CI:1.02–1.10, p = 0.006). In the subgroup analysis by treatment, there was a significant association between physical QoL and mortality risk in both HSCT (HR:1.03, 95% CI:1.00–1.06, p = 0.02) and chemotherapy (HR:1.08, 95% CI:1.00–1.17, p = 0.04, I2 = 66%), respectively. There were no significant differences between the subgroups (p = 0.24) (Fig. 3).
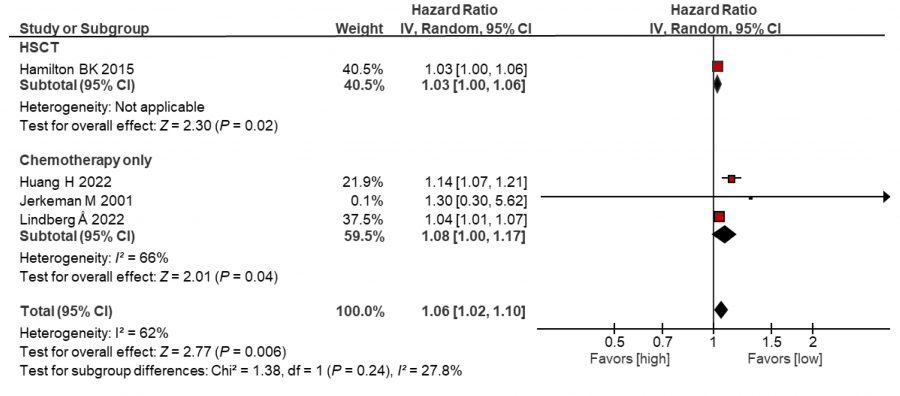
Fig. 3.
Meta-analysis of the association between physical QoL and mortality risk in patients with hematological malignancies
Association between emotional QoL and mortality risk
One study on HSCT was included in a random-effects meta-analysis. There was no significant association between emotional QoL and mortality risk (HR:1.00, 95% CI:0.96–1.04, p = 1.00) (Fig. 4).

Fig. 4.
Meta-analysis of the association between emotional QoL and mortality risk in patients with hematological malignancies
Association between role QoL and mortality risk
One study on chemotherapy was included in a random-effects meta-analysis. There was a significant association between role QoL and mortality risk (HR:1.02, 95% CI:1.00–1.04, p = 0.009) (Fig.5).

Fig. 5.
Meta-analysis of the association between role QoL and mortality risk in patients with hematological malignancies
Association between social QoL and mortality risk
Two studies were included in a random-effects meta-analysis. Overall, there was a significant association between social QoL and mortality risk (HR:1.02, 95% CI:1.00–1.03, p = 0.04). In the subgroup analysis by treatment, although there was no significant association between social QoL and mortality risk in HSCT (HR:1.00, 95% CI:0.97–1.04, p = 1.00), a significant association was observed in chemotherapy (HR:1.02, 95% CI:1.00–1.04, p = 0.009). There were no significant differences between the subgroups (p = 0.30) (Fig. 6).
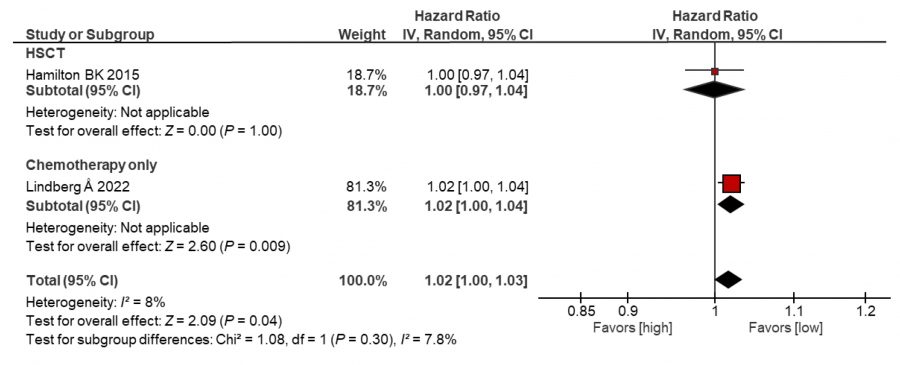
Fig. 6.
Meta-analysis of the association between social QoL and mortality risk in patients with hematological malignancies
Discussion
In this meta-analysis, we focused on whether QoL before treatment, including HSCT and chemotherapy, affects OS in patients with hematological malignancy. The main findings of this systematic review and meta-analysis were as follows. Global QoL and physical QoL were associated with prognosis, and significant associations were also observed in the subgroup analyses of HSCT and chemotherapy. Role QoL showed an association with OS in the studies involving chemotherapy patients, although no such association was found among the HSCT patients. No relationship between social QoL and OS was observed in the HSCT studies, but one such relationship was observed in the chemotherapy studies. Finally, emotional QoL did not exhibit a significant association with OS in any of the studies.
Traditionally, the survival rates of cancer patients have been attributed to factors related to the cancer itself, such as stage and site, as well as patient-related factors like age, health status, and treatment resistance37-39). Performance status (PS) has been particularly recognized as a convenient assessment scale for understanding a patient’s overall condition, often guiding treatment decisions due to its association with treatment-related adverse events40). Furthermore, PS has been reported to be associated with survival rates in various types of cancer41-44), and has also been identified as a factor influencing survival in patients with hematological malignancies45-48). The present study revealed that pretreatment global QoL significantly influenced survival rates. Jerkeman et al.34) reported that, among aggressive lymphoma patients undergoing chemotherapy, pretreatment global QoL emerged as a significant prognostic factor for survival, surpassing PS. However, given the limited number of patients with PS > 1 in their study, it was suggested that evaluating global QoL rather than PS could be useful in predicting survival, especially among younger patients or patients with good overall health status. Similarly, Jung et al.35) suggested that diffuse large B-cell lymphoma patients with low pretreatment global QoL exhibited poor resistance to chemotherapy, leading to decreased OS, regardless of age or PS. Moreover, patients who died due to treatment-related complications had lower pretreatment global QoL scores, indicating increased treatment-associated mortality. Thus, the results of the present review indicate that pretreatment global QoL affects OS in patients undergoing either HSCT or chemotherapy alone, underscoring its recognition as a valuable factor for improving OS. Furthermore, healthcare providers should acknowledge that pretreatment global QoL may offer superior prognostic capabilities compared to factors previously reported to influence survival rates. However, whether this applies universally across hematological malignancies or only to specific patient groups remains uncertain due to insufficient evidence, highlighting the need for further research in this area.
Among the QoL parameters, both global QoL and physical QoL were associated with favorable OS in patients undergoing HSCT or chemotherapy. The impact of pretreatment QoL on OS has also been observed in other cancer types49-51). While pretreatment global QoL may be crucial in predicting survival rates, detailed evaluation of physical function is also deemed necessary. Global QoL encompasses various factors, including age, cancer stage, nutrition, and activity level, which may act as surrogate markers for OS. Moreover, patients with hematologic malignancies are more likely to be younger at the time of diagnosis compared to those with other cancers, and those undergoing HSCT are often also younger. The decision-making process in cancer treatment varies by age, with young adult patients more likely to undergo aggressive treatments aimed at prolonging life52). Given the younger demographic often seen in patients with hematologic malignancies, it is expected that they would likely be able to maintain relatively good general QoL and physical well-being prior to treatment. Physical function has also been associated with post-HSCT prognosis53), suggesting that patients with better physical function before treatment may have higher physical QoL, enabling them to undergo more aggressive treatments that could, in turn, improve OS. Hamilton et al.31) reported, that among HSCT patients, physical function, particularly physical well-being, correlated with OS, although no association with non-relapse mortality was observed. The underlying reasons for the differing associations between QoL and both survival rates and non-relapse mortality remain unclear, but physical function may be influenced not only by cancer-specific symptoms and physical characteristics, but also by comorbidities, as noted in reports by Kurosawa et al32). However, despite the influence of comorbidities, if the evaluation of physical QoL as a QoL parameter enables the prediction of OS, it should be assessed at the pre-transplantation stage. Similarly, in chemotherapy patients, physical QoL among QoL parameters influenced OS. Huang et al.33) and Lindberg et al.36) reported that, among QoL parameters, physical QoL was associated not only with OS but also with progression-free survival (PFS). Hematological malignancy patients exhibit decreased muscle strength, overall endurance, and skeletal muscle mass even before transplantation or chemotherapy, with differences in physical function observed based on hemoglobin levels, an indicator of anemia24,54-56). Moreover, treatment-related declines in physical function have been observed2,57-59). Thus, cancer itself and its treatment may precipitate decreases in physical function, emphasizing the need for healthcare providers to focus not only on the global QoL but also on physical QoL before treatment initiation. Chemotherapy alone had a higher HR for OS compared to HSCT. It is possible that the HSCT patients may have had a decline in physical function due to prior experience with various treatments and associated adverse events, possibly leading to a lower HR for OS compared to chemotherapy-only patients. Assessing physical QoL as a QoL parameter is straightforward and feasible for healthcare providers, and combining actual physical function evaluations, such as comorbidities, muscle strength, and overall endurance, may not only enhance the predictive accuracy of individual patient OS and PFS, but also contribute to comprehensive treatment strategies.
Moreover, role QoL and social QoL among the QoL parameters did not show a significant association with OS in the HSCT studies, whereas they exhibited a significant association in the chemotherapy studies. In HSCT, patients undergo several rounds of treatment in the stages leading up to transplantation. In addition, the aggressive treatment of transplantation often results in hospitalization and aseptic management due to marked immune compromise. On the other hand, chemotherapy-only treatment often follows an outpatient course. In addition, since most patients tend to live at home during the pre-treatment phase of chemotherapy, it is likely that most of them have a normal social life. In outpatient treatment, patients are expected to undergo treatment while fulfilling: their social roles, such as performing household chores like cooking and laundry; their employment responsibilities; and their community engagements. Therefore, in patients undergoing HSCT, the opportunities to fulfill the above roles and social aspects decrease with hospitalization, and there is a potentially significant association with OS observed in studies focusing on the use of chemotherapy in patients who are predominantly home-based. Additionally, patients with strong psychosocial support systems tend to have better health outcomes, as these factors are known to enhance resilience and treatment adherence60). When role and social aspects of QoL are high before treatment, it is likely that a robust psychosocial support system is already in place, which could contribute to a favorable treatment course and potentially extend OS. Conversely, when physical, role, and social QoL are low prior to treatment, greater support may be needed during the treatment process. In some cases, the lack of sufficient support may hinder the continuation of aggressive treatment, potentially leading to a decrease in OS. Lindberg et al.36) reported that according to their multivariate analysis, decreases in physical QoL and role QoL before treatment were associated with decreased OS. From the univariate analysis results, associations with OS were also found for social QoL, with correlations observed between role QoL and PFS as well as between role QoL and PS. While fewer studies have reported associations with OS compared to global QoL and physical QoL, it is crucial to recognize role QoL and social QoL as important prognostic factors. These QoL reflect roles and sociability in daily life activities and social interactions. Reports have indicated that role and social QoL are lower in hematological malignancy patients compared to healthy individuals61,62). Patients with hematological malignancies develop the condition at a younger age compared to other types of cancer, and it has been reported that the lack of social support negatively affects QoL63). Treatment-related declines in physical function restrict subsequent social life. Roles and social QoL are not only issues related to daily life and social activities, but may also be factors involved in OS. Ueno et al.64) suggested that interdisciplinary care in cancer treatment should be provided by teams with roles such as active care staff who provide medical care to patients, base support care staff who support patient needs, and community support staff, who need to cooperate with each other to provide patient-centered care. From the pretreatment stage, it may be necessary to evaluate the QoL from various perspectives, including not only global QoL, but also physical, role, and social QoL, in order to improve patient prognosis while considering the involvement of healthcare professionals and regional resources. Emotional QoL was not associated with either HSCT or chemotherapy. Patients with hematologic malignancies often experience psychological stress because they are treated in private rooms for aseptic management and are required to take strict infection control measures. Therefore, emotional QoL is considered one of the important aspects of QoL for HSCT patients; however, only one paper on HSCT was included in the present study, which may not have led to the conclusion of an association with OS.
This review has several limitations. Firstly, although this review utilized relatively large databases such as CINAHL, PubMed/MEDLINE, and Scopus, there may be other databases with relevant articles. Secondly, only six studies were selected for this review, with varied QoL assessment tools including EORTC-QLQ-C30, EQ-5D, and FACT-G, contributing to heterogeneity due to differences in evaluation items and the limited number of articles. Therefore, the need for further research must be emphasized to provide clearer evidence for the present results. Thirdly, this review included hematological malignancy patients with various disease states who had been treated with different methods such as HSCT and chemotherapy, potentially overlooking differences in QoL due to due to these variations. Finally, based on the results of the present study, it would be a more clinically relevant assessment if the level of QOL could be quantified and consistently assessed by specialists in multiple professions. However, that was not within the scope of the present study, and quantification and scoring of QOL evaluations should be investigated in the future.
Conclusion
In the present review, it was revealed that pretreatment global QoL and physical QoL were associated with OS in patients with hematological malignancy treated with HSCT or chemotherapy. In addition, role QoL and social QoL were found to be associated with OS in chemotherapy patients, with different factors associated with OS depending on treatment. Evaluating QoL overall and by parameter from the pretreatment stage enables the prediction of OS, thereby suggesting the potential of supportive therapy during and after treatment. However, many mechanisms regarding how pretreatment QoL influences OS remain unclear, emphasizing the need for further research.
Author contributions
All authors contributed to the study conception and design. Material preparation and data collection and analysis were performed by KO, SM, JN, JI, TO, KS, TT, and TF. The first draft of the manuscript was written by KO, and all authors commented on intermediate versions of the manuscript. All authors read and approved the final manuscript.
Acknowledgements
The authors gratefully acknowledge the support of the members of the Cancer Rehabilitation Laboratory. Without their cooperation, this study would not have been possible.
Declarations
Ethical approval
Not applicable
Funding
None