Rectal cancer is one of the leading causes of cancer mortality worldwide1), for which treatment to improve outcomes is demanding. Radical resection, with total mesorectal excision (TME) / tumor-specific mesorectal excision (TSME), is generally accepted to be first-line treatment for resectable rectal cancer in Japan2). TME/TSME surgery for rectal cancer is challenging, due to a narrow pelvic operating field and the need to preserve autonomic nerve function and mesorectal fascia integrity. In Japan, lateral pelvic lymph node dissection (LPND) is recommended for rectal cancers with distal margins beyond the peritoneal reflection and depth beyond the propria muscle2), making surgery even more difficult. In the late 19th century, Gerota et al. revealed the presence of lateral lymphatic flow in the distal rectum toward the pelvic wall3). From the 1980s, LPND was developed and established mainly in Japan4,5) where a local recurrence rate of less than 10% was achieved, ahead of Western countries. However, the initial LPND technique was reported to cause a high incidence of postoperative sexual and urinary dysfunction, prompting the development of autonomic nerve-preserving LPND techniques6,7). Currently, autonomic nerve-preserving LPND is widely accepted as one of the standardized surgical procedures for lower rectal cancer, mainly in East Asia. Regarding oncological outcome of autonomic nerve-preserving LPND, JCOG02128), a Japanese nation-wide randomized controlled trial, demonstrated a high rate of local control, although it failed to demonstrate any survival benefit. Therefore, the clinical efficacy of autonomic nerve-preserving LPND is not yet fully accepted worldwide. Furthermore, a long-recognized Western standard of care to control local tumor growth has been preoperative chemoradiotherapy (CRT). However, local tumor control was reported to be not completely achieved by preoperative CRT, and evidence is accumulating in support of LPND, even in the West, especially in cases where lateral lymph node metastases are already present prior to the initial treatment9,10).
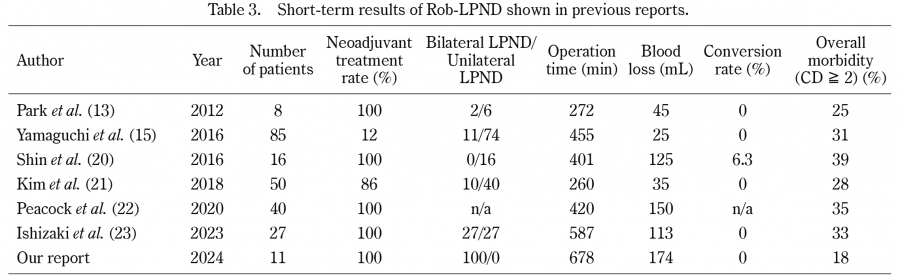
LPND started as an open technique, and, as surgery has evolved, it has shifted to a laparoscopic approach11,12). As compared to open LPND, laparoscopic-LPND (Lap-LPND) is associated with longer operative time, but less blood loss, with comparable degrees of postoperative complications. The first robotic LPND (Rob-LPND) was reported in 201213), with a belief emerging that Rob-LPND offers more precise manipulation in a narrow pelvis, since robot-assisted techniques can provide a stable and magnified view, with multidirectional articulation functions, motion scale, and elimination of tremor. There is still limited information to support Rob-LPND, mainly in East Asia14-17), where it is at least comparable to Lap-LPND in short-term outcomes. Our hospital began Rob-LPND in 2021, from which we herein report its short-term outcomes in comparison with those of Lap-LPND.