Abstract/References
Struma ovarii with massive ascites mimicking ovarian carcinoma treated with conservative laparoscopic surgery: a case report
Riho Yazawa, Hiroyuki Yazawa, Kaoru Fukuda, Miki Ohara
Author information
- Riho Yazawa
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital - Hiroyuki Yazawa
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital - Kaoru Fukuda
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital - Miki Ohara
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
Abstract
Struma ovarii is a rare taratoma that accounts for 0.5-1% of all ovarian tumors. It is sometimes difficult to differentiate struma ovarii from ovarian carcinoma. We encountered a case of struma ovarii that was suspected to be malignant due to the accumulation of massive ascites and an elevated CA125 level. It was successfully treated with laparoscopic surgery.
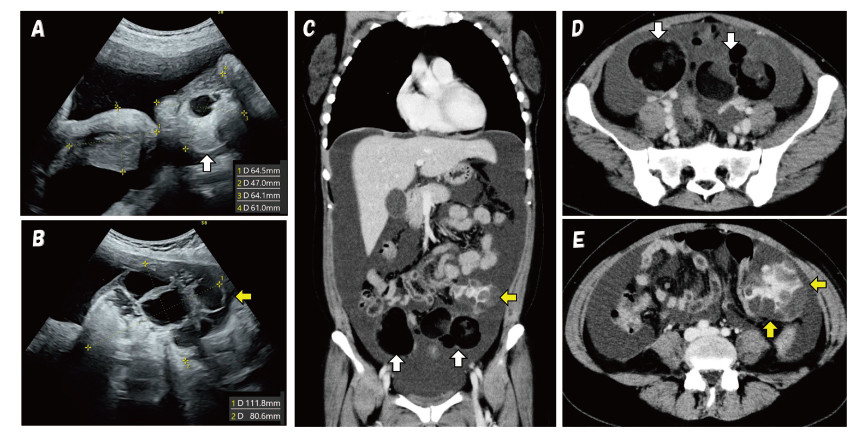
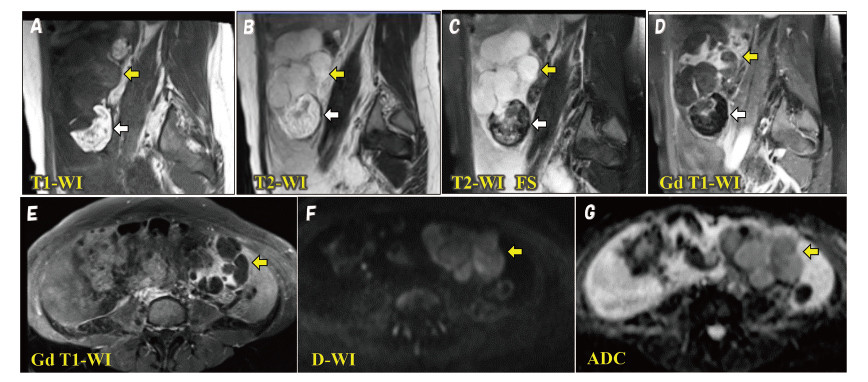
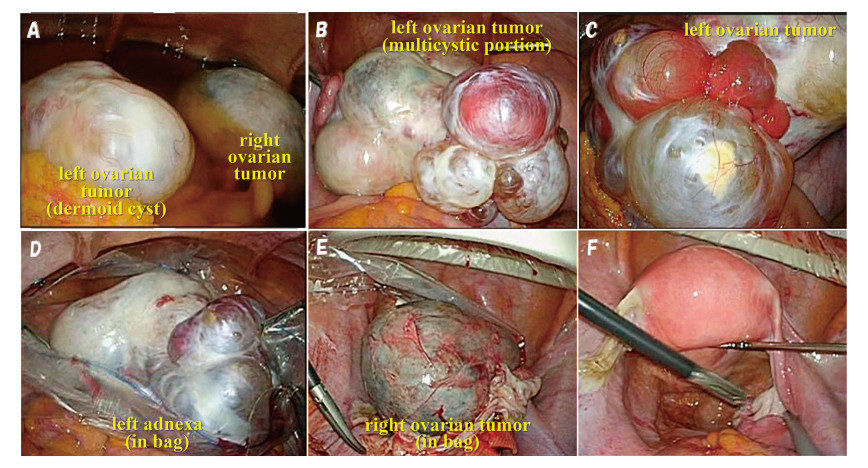
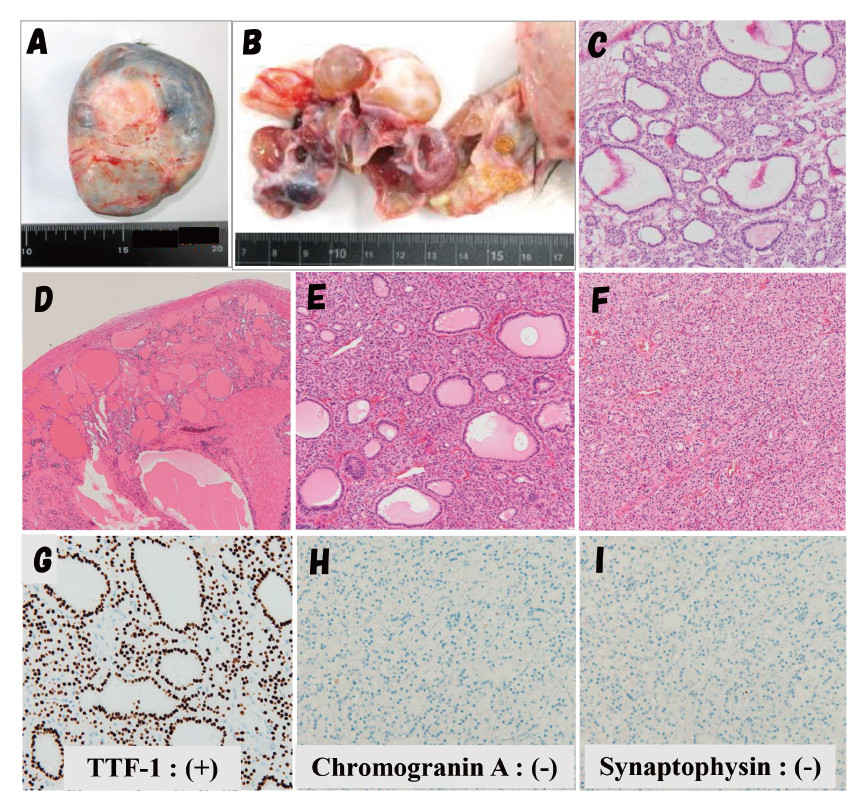
A 37-year-old nulliparous woman consulted a local physician with a chief complaint of abdominal distention. Computed tomography (CT) of the abdomen revealed a pelvic tumor with a large amount of ascites. She was referred to our department. Contrast-enhanced magnetic resonance imaging (MRI) and CT showed bilateral ovarian tumors with multicystic and solid components. CA125 level was markedly elevated. Two cytological examinations of ascites showed no malignant cells. Preoperatively, malignancy was strongly suspected, but considering the possibility of a benign ovarian tumor, laparoscopic surgery was scheduled. During laparoscopic surgery, 4,850 mL of ascites were aspirated, and the left adnexa was removed. Intraoperative rapid pathology suggested struma ovarii with no evidence of malignancy. Postoperative pathology showed mature teratoma and struma ovarii.
Although struma ovarii is benign in 90-95% of cases, there have been scattered case reports in which suspected malignancy led to unnecessary or excessive surgery. We propose that appropriate preoperative imaging and accurate intraoperative rapid pathology can prevent excessive surgery, conservative or laparoscopic excisions should be considered.
References
- 1.Wee JYS, Li X, Chern BSM, Chua ISY. Struma ovarii:management and follow-up of a rare ovarian tumour.
- 2.Yoo SC, Chang KH, Lyu MO, et al. Clinical characteristics of struma ovarii. J Gynecol Oncol, 19:135-138, 2008.
- 3.Jiang W, Lu X, Zhu ZL, et al. Struma ovarii associated with pseudo-Meigs’ syndrome and elevated serum CA125:a case report and review of the literature. J Ovarian Res, 3:18, 2010.
- 4.Yadav S, Tomar R, Verma N, Khurana N, Triathi R. Struma ovarii with pseud-Meigs’ syndrome and raised cancer antigen-125 levels masquerading as an ovarian carcinoma. Case report and literature review. Sultan Qaboos University Med J, 17:229-233, 2017.
- 5.Guida M, Mandato VD, Di Spiezio Sardo A, Carlo C, Giordano E, Nappi C. Coexistence of Graves’ disease and benign struma ovarii in a patient with marked ascites and elevated CA125 levels. J Endocrinol Invest, 28:827-830, 2005.
- 7.Checrallah A, Medlej R, Saade C, Khayat G, Halaby G. Malignant struma ovarii:an unusual presentation. Thyroid, 11:889-892, 2001.
- 10.Singh P, Lath N, Shekhar S, et al. Struma ovarii: A report of three cases and literature of review. J Midlife Health, 9: 225-229, 2018.
- 11.Ikeuchi T, Koyama T, Tamai K, et al. CT and MRI features of struma ovarii. Abdom Imaging, 37: 905-910, 2012.
- 12.Meigs JV. Fibroma of the ovary with ascites and hydrothorax; Meigs’ syndrome. AM J Obstet Gynecol, 67: 962-985, 1954.
- 14.Jin C, Dong R, Bu H, et al. Coexistence of benign struma ovarii, pseudo-Meigs’ syndrome and elevated serum CA125: Case report and review of the literature. Oncol Letter, 9: 1739-1742, 2015.
Figures