Abstract/References
A case of polypoid endometriosis mimicking advanced ovarian carcinoma with rapid growth, invasion, and dissemination
Hiroyuki Yazawa, Riho Yazawa, Kaoru Fukuda, Miki Ohara
Author information
- Hiroyuki Yazawa
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital - Riho Yazawa
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital - Kaoru Fukuda
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital - Miki Ohara
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
Abstract
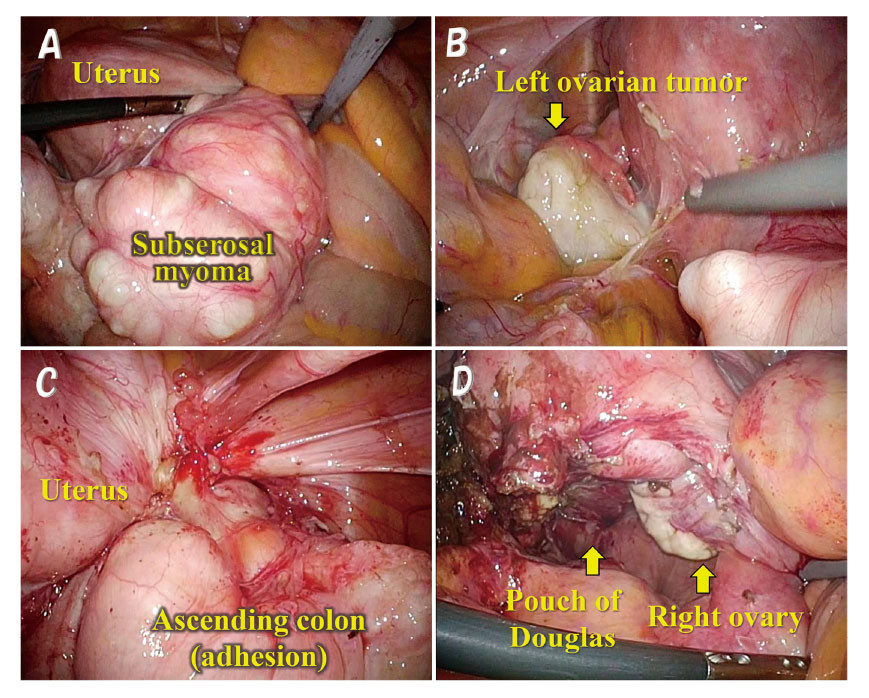
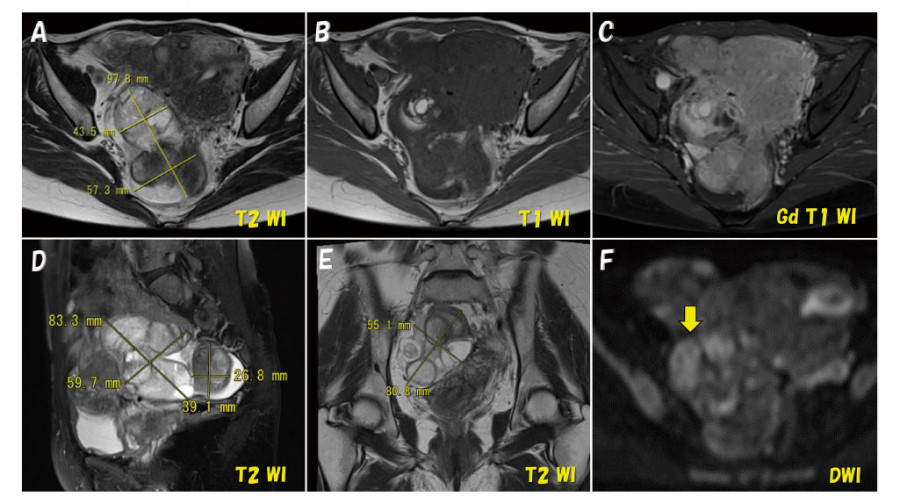
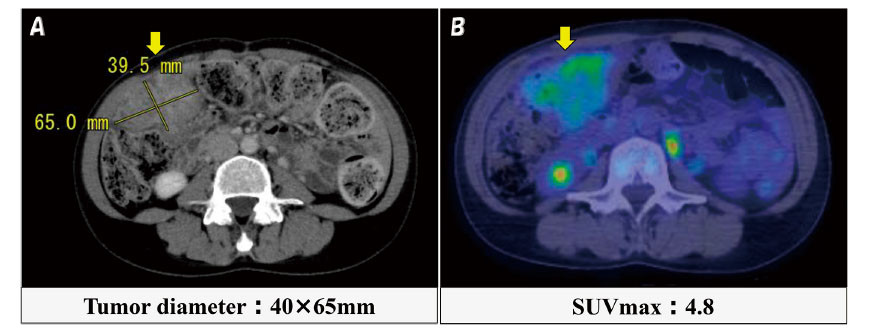
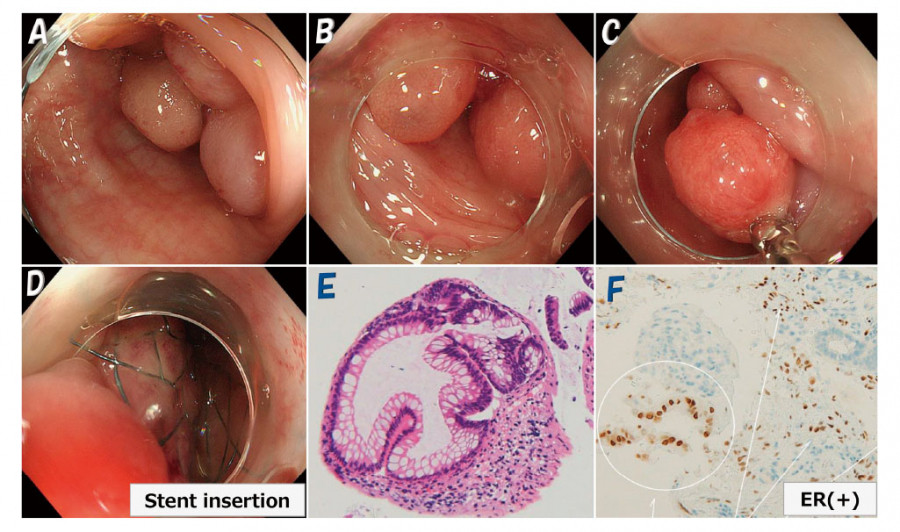
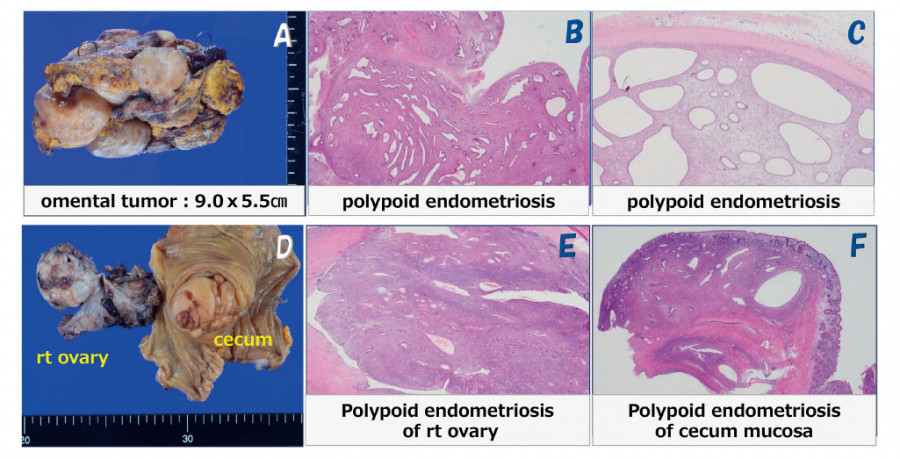
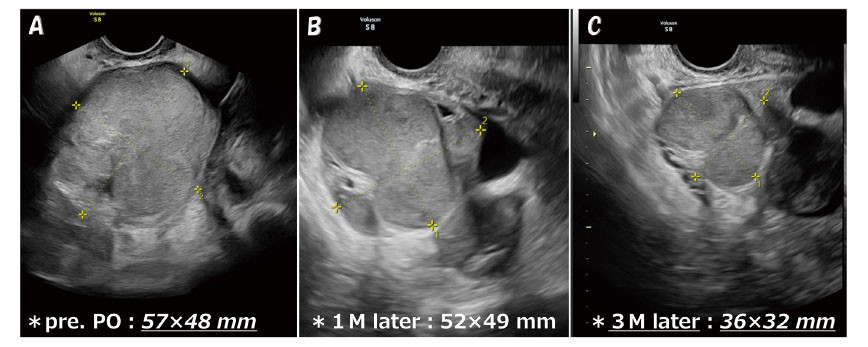
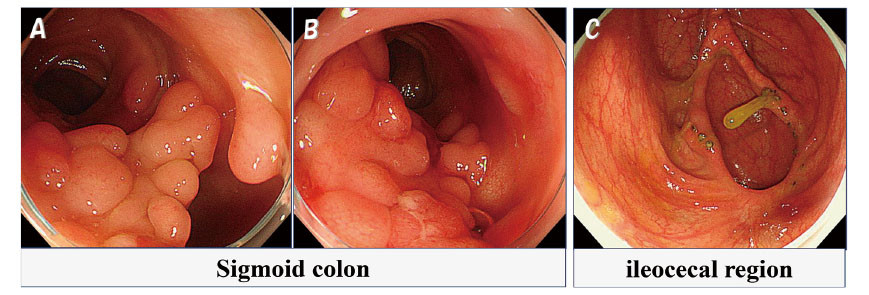
Polypoid endometriosis is a rare form of endometriosis characterized by polypoid masses that histologically often resemble endometrial polyps. We report a case of rapidly progressing polypoid endometriosis that was preoperatively assumed to be advanced ovarian cancer. A 46-year-old woman, para 0, underwent laparoscopic myomectomy and left adnexectomy for uterine fibroids and a left ovarian endometrial cyst after administration of gonadotropin releasing hormone (GnRH) agonist for 4 months. Eleven months postoperatively, rapid right ovarian enlargement occurred. CT and MRI (both contrast-enhanced) showed masses in the right adnexa, cecum, sigmoid colon, and omentum, and PET-CT demonstrated increased uptake, suggesting ovarian cancer and peritoneal dissemination. The patient later developed intestinal obstruction, and colonoscopy revealed multiple polypoid lesions in the sigmoid colon. The omental tumor and right adnexa were biopsied during exploratory laparotomy, and diagnosed as polypoid endometriosis with no malignancy by permanent pathology. The right adnexal tumor shrunk markedly after 4 months of GnRH antagonist treatment. Second laparotomy was then performed for right adnexal tumor resection and ileocecectomy. Pathological examination revealed polypoid endometriosis extending from the ovary to the cecal mucosa. The patient has been asymptomatic for over 1 year postoperatively. The sigmoid colon tumor shrunk but is still present.
Polypoid endometriosis predominantly affects the ovaries, colon, peritoneum, and omentum of patients in their 40s and 50s. It is a benign disease but is often difficult to distinguish from malignancy preoperatively because it rapidly forms numerous solid lesions. Although polypoid endometriosis is rare, with no specific imaging findings, including it in a differential diagnosis may facilitate preoperative identification.
References
- 7.Kim JY, Song TJ, Choi HK, Shim JY. Multifocal polypoid endometriosis mimicking malignancy in a young woman with a history of hormonal treatment. J Pathol Transl Med, 49:418-420, 2015.
- 9.Choi IH, Jin SY, Jeen YM, Lee JJ, Kim DW. Tamoxifen-associated polypoid endometriosis mimicking an ovarian neoplasm. Obstet Gynecol Sci, 58:327-330, 2015.
- 11.Chang CK, Chen P, Leu FJ, Lou SMA. Florid polypoid endometriosis exacerbated by tamoxifen therapy in breast cancer. Obstet Gynecol, 102:1127-1130, 2006.
- 13.Ferno M, Baldetorp B, Bendahl PO, et al. Recurrence-free survival in breast cancer improved by adjuvant tamoxifen-especially for progesterone receptor positive tumors with a high proliferation. Brest Cancer Res Treat, 36:23-34, 1995.
- 14.Hann LE, Giess CS, Bach AM, Tao Y, Baum HJ, Barakat RR. Endometrial thickness in tamoxifen-treated patients:correlation with clinical and pathological findings. Am J Roentgenol, 168:657-661, 1997.
- 17.Risum S, Hogdall C, Loft A, et al. The diagnostic value of PET/CT for primary ovarian cancer- a prospective study. Gynecol Oncol, 105:145-149, 2007.
Figures (7)