Abstract/References
Association between subjective economic status and refusal of life-prolonging treatment: a cross-sectional study using content analysis with stratified random sampling
Hideaki Kasuga, Shota Endo, Yusuke Masuishi, Tomoo Hidaka, Takeyasu Kakamu, Keiko Saito, Koichi Abe, Tetsuhito Fukushima
Author information
- Hideaki Kasuga
Department of Hygiene and Preventive Medicine, Fukushima Medical University - Shota Endo
Department of Hygiene and Preventive Medicine, Fukushima Medical University - Yusuke Masuishi
Department of Hygiene and Preventive Medicine, Fukushima Medical University - Tomoo Hidaka
Department of Hygiene and Preventive Medicine, Fukushima Medical University - Takeyasu Kakamu
Department of Hygiene and Preventive Medicine, Fukushima Medical University - Keiko Saito
Koriyama City Public Health Center - Koichi Abe
Koriyama City Public Health Center - Tetsuhito Fukushima
Department of Hygiene and Preventive Medicine, Fukushima Medical University
Abstract
Introduction: Older adults tend to refuse life-prolonging treatment for various reasons, and it is important to respect their choice of treatment at the end-of-life stage. The present study examines the associations of subjective economic status and gender with reasons for refusal of life-prolonging treatment in older adults in general population.
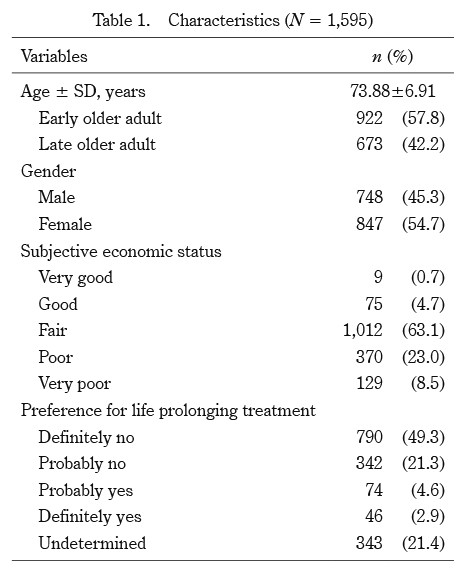
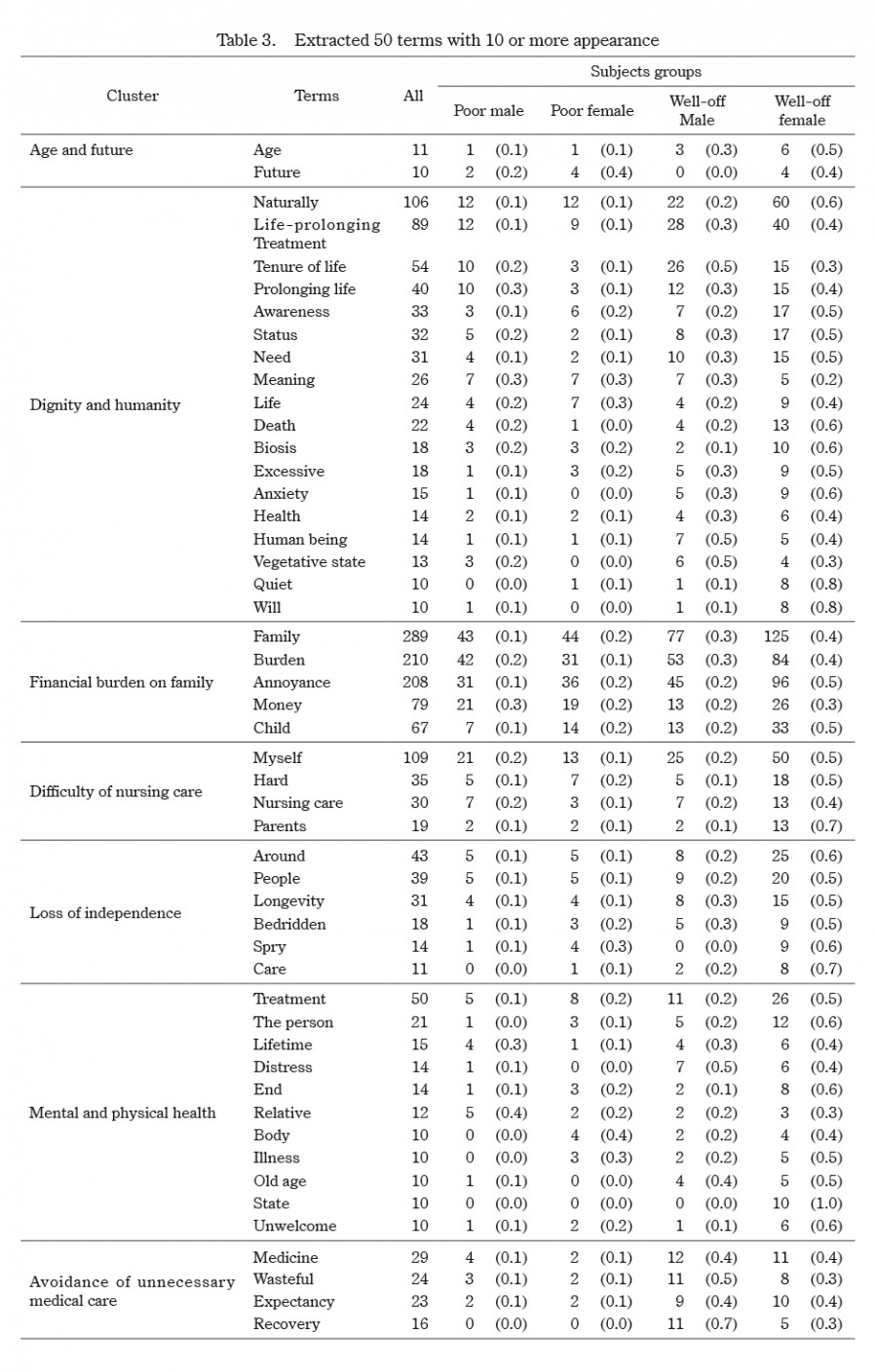
Methods: In this cross-sectional study, using stratified random sampling, 1,595 older adults living in Koriyama City, Japan, as of 2016, completed self-administered questionnaires on subjective economic status and preference for life-prolonging treatment, with free-description regarding reasons for refusal. We analyzed the associations between the combination of subjective economic status and gender with frequently mentioned terms and their clusters regarding such reasons, using χ2 test, content analysis, text mining and hierarchical cluster analysis.
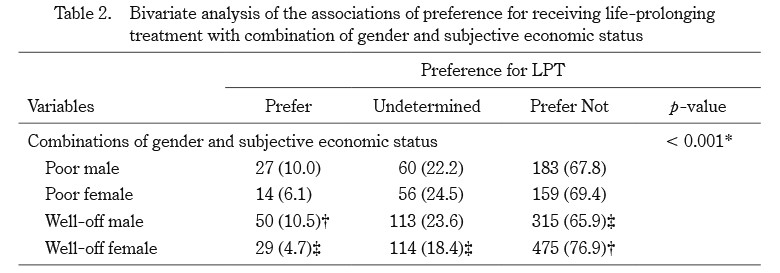
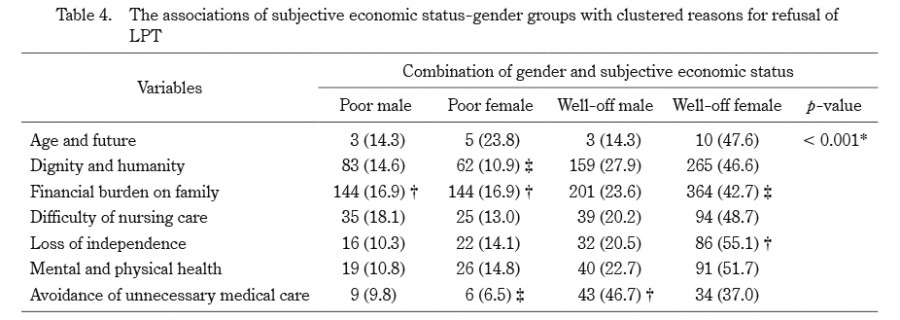
Results: The combinations of subjective economic status and gender were significantly associated with clustered reasons for refusal of life-prolonging treatment (p < 0.01). The reasons frequently mentioned were: ‘avoidance of unnecessary medical care’ and ‘dignity’ in well-off females; and ‘financial burden on family’ in poor males.
Conclusions: Our findings suggest that older adults who at first glance appear to be freely refusing life-prolonging treatment, may have their decision making restricted through economic constraints.
References
- 1.Bosshard G, Zellweger U, Bopp M, et al. Medical End-of-Life Practices in Switzerland: A Comparison of 2001 and 2013. JAMA Intern Med, 176:555-556, 2016.
- 2.Clarke G, Fistein E, Holland A, Barclay M, Theimann P, Barclay S. Preferences for care towards the end of life when decision-making capacity may be impaired:A large scale cross-sectional survey of public attitudes in Great Britain and the United States. PLoS One, 12:e0172104, 2017.
- 3.Mori M, Morita T. Advances in Hospice and Palliative Care in Japan:A Review Paper. Korean J Hosp Palliat Car, 19:283-291, 2016.
- 6.van Wijngaarden E, Goossensen A, Leget C. The social-political challenges behind the wish to die in older people who consider their lives to be completed and no longer worth living. J Eur Soc Policy, 28:419-429, 2018.
- 8.Crawley L, Payne R, Bolden J, Payne T, Washington P, Williams S. Palliative and end-of-life care in the African American community. JAMA, 284: 2518-2521, 2000.
- 9.Borum ML, Lynn J, Zhong Z. The effects of patient race on outcomes in seriously ill patients in SUPPORT:an overview of economic impact, medical intervention, and end-of-life decisions. J Am Geriatr Soc, 48:194-198, 2000.
- 12.Halvorsen K, Førde R, Nortvedt P. Value choices and considerations when limiting intensive care treatment:a qualitative study. Acta Anaesthesiol Scand, 53:10-17, 2009.
- 13.Arber S, Vandrevala T, Daly T, Hampson S. Understanding gender differences in older people’s attitudes towards life-prolonging medical technologies, J Aging Stud, 22:366-375, 2008
- 15.Hidaka T, Endo S, Kasuga H, et al. Disparity in pre-emptive end-of-life conversation experience caused by subjective economic status among general Japanese older adults:a cross-sectional study with stratified random sampling, BMJ Open, 9:e031681, 2019.
- 19.Seale C, Addington-Hall J. Dying at the best time. Soc Sci Med, 40:589-595, 1995.
- 20.Bhandari TR, Kutty VR, Ravindran TK. Women’s Autonomy and Its Correlates in Western Nepal: A Demographic Study. PLoS One, 11(1):e01474732016.
- 21.Nilsson ME, Maciejewski PK, Zhang B, et al. Mental health, treatment preferences, advance care planning, location, and quality of death in advanced cancer patients with dependent children. Cancer, 115:399-409, 2009.
- 22.Barnato AE, Anthony DL, Skinner J, Gallagher PM, Fisher ES. Racial and ethnic differences in preferences for end-of-life treatment. J Gen Intern Med, 24:695-701, 2009.
- 23.Smith JP. Healthy bodies and thick wallets:the dual relation between health and economic status. J Econ Perspect, 13:144-166, 1999.
Figures