Abstract/References
Development of a self-administered questionnaire for the screening of cervical myelopathy. Part 2, investigation of its characteristics in surgical cases
Hiroshi Kobayashi, Koji Otani, Junichi Handa, Kinshi Kato, Kazuyuki Watanabe, Takuya Nikaido, Shoji Yabuki, Shin-ichi Konno
Author information
- Hiroshi Kobayashi
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine - Koji Otani
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine - Junichi Handa
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine - Kinshi Kato
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine - Kazuyuki Watanabe
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine - Takuya Nikaido
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine - Shoji Yabuki
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine - Shin-ichi Konno
Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine
Abstract
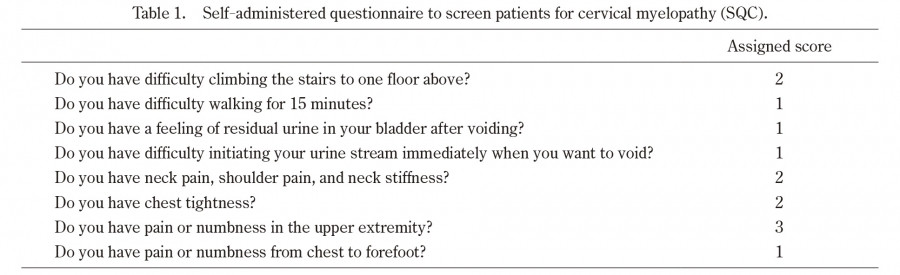
Background: Our previous report described the development of a self-administered questionnaire to screen patients for cervical myelopathy (SQC). For clinical application, the characteristics of the SQC should be verified.
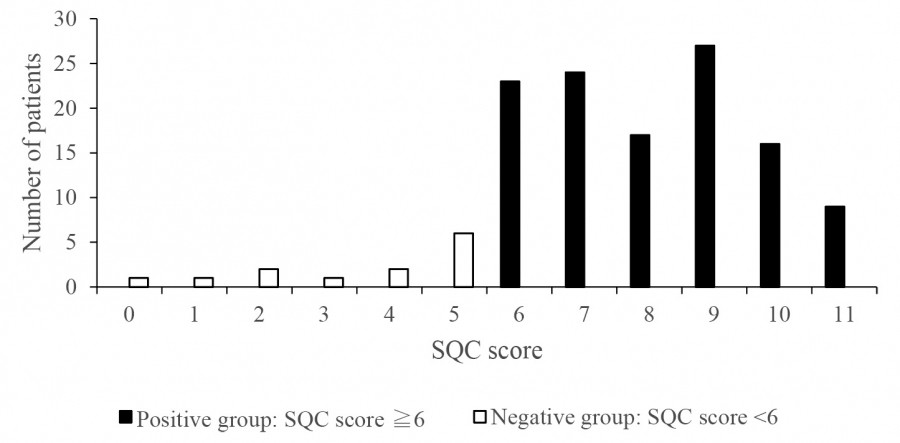
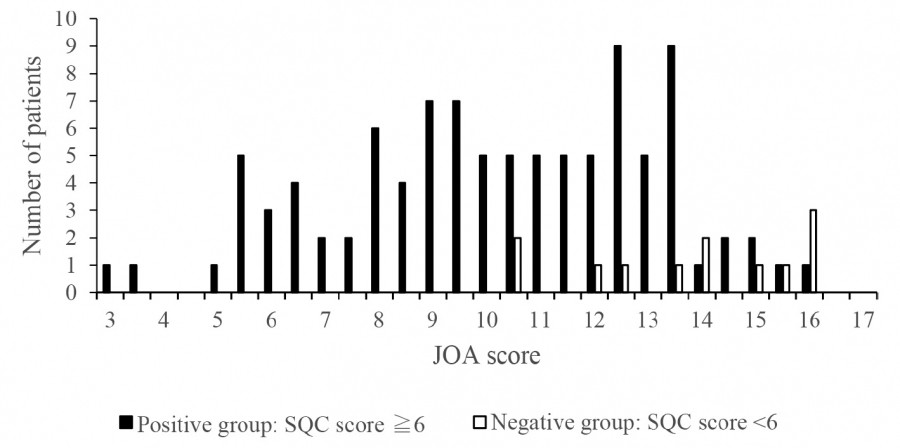
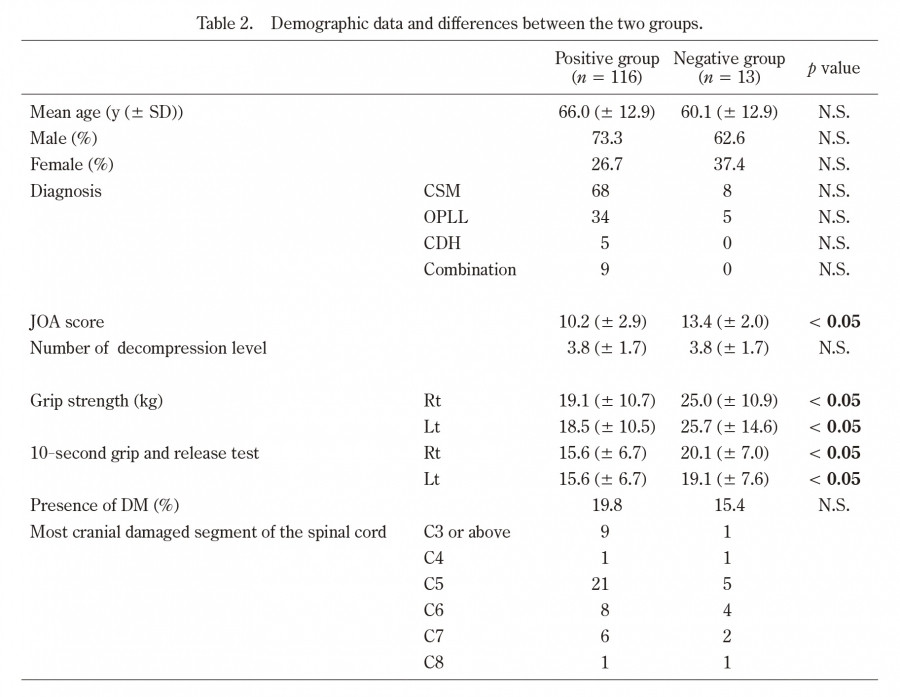
Methods: Participants comprised 129 patients (94 men, 35 women) with cervical myelopathy who underwent operative treatment. SQC score was calculated before surgery and patients were divided into a positive group (score ≥6) and negative group (score <6). Sex, age, pathologies of cervical myelopathy, Japanese Orthopaedic Association (JOA) score, 10-s grip-and-release test (10-s test), grip strength, number of levels decompressed, most cranial level of damage, and presence of diabetes mellitus (DM) were compared between groups.
Results: The sensitivity was 89.9% with 116 positive cases and 13 negative cases (10.1%). JOA score was significantly higher and 10-s test and grip strength significantly better in the negative group than in the positive group. No significant differences in sex, age, pathologies of cervical myelopathy, number of spinal levels decompressed, most rostral level of damage, or presence of DM were seen between groups.
Conclusions: Screening for cervical myelopathy using SQC had a high sensitivity of 89.9%. However, SQC should be used with caution because it may miss mild cervical myelopathy with low JOA scores.
References
- 1.Nurick S. The pathogenesis of the spinal cord disorder associated with cervical spondylosis. Brain, 95(1): 87-100, 1972.
- 2.Kikuchi S, Otani K, Sekiguchi M, Sekiguchi Y, Konno S. Development of a self-administered questionnaire to screen patients for cervical myelopathy. BMC Musculoskeletal Disord, 22(11): 268-273, 2010.
- 6.Revised Japanese Orthopaedic Association scores for cervical myelopathy. J Jpn Orthop Assoc, 68: 490-503 (in Japanese), 1994.
- 7.Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K. Myelopathy hand. New clinical signs of cervical cord damage. J Bone Joint Surg Br, 69(2): 215-219, 1987.
- 10.Young WF. Cervical spondylotic myelopathy: A common cause of spinal cord dysfunction in older persons. Am Fam Physician, 62(5): 1064-1073, 2000.
- 11.Wu JC, Ko CC, Yen YS, Huang WC, Chen YC, Liu L, Tu TH, Lo SS, Cheng H. Epidemiology of cervical spondylotic myelopathy and its risk of causing spinal cord injury: a national cohort study. Neurosurg Focus, 35(1): E10, 2013.
- 12.Uchida K, Nakajima H, Sato R, Kokubo Y, Yayama T, Kobayashi S, Baba H. Multivariate analysis of the neurological outcome of surgery for cervical compressive myelopathy. J Orthop Sci, 10(6): 564-573, 2005.
Figures