Study design and sample
In this cross-sectional study, a stratified random sampling method was used to select 3,000 participants from the population of Koriyama City in Fukushima Prefecture, Japan, as follows. First, of the total elderly population of Koriyama City, those aged 65 years or older, (84,030; 37,382 males and 46,648 females) who were not receiving nursing care as of November 1, 2016, were selected from the Japanese long-term care insurance system registry and excluded, bringing the number down to 78,821 (33,958 males and 44,863 females).
Next, the potential participants were stratified by gender and location, according to the 20 sub regions outlined by Koriyama City’s administrative boundaries. Sampling weights were then applied to adjust for gender and region distributions proportionate to the population size of elderly people. Finally, 1,301 males (43.4%) and 1,699 females (56.6%) were enrolled in the study.
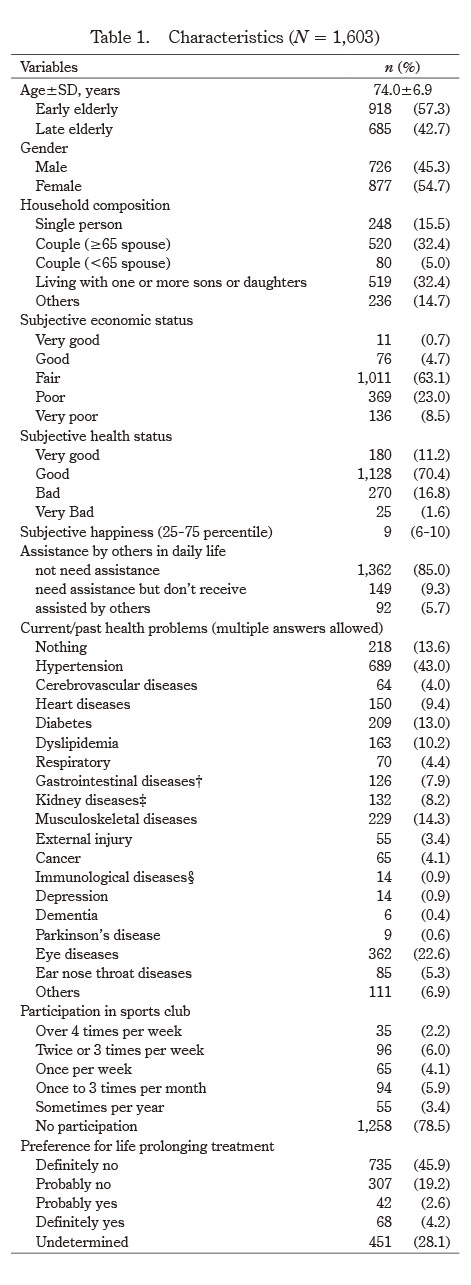
In January 2017, we distributed questionnaires to the 3,000 participants, which included items covering basic attributes, participation in sports club activities, and decision-making about treatment at the EOL stage. We also asked if the patient completed the questionnaire themselves and if not, by whom. Participants gave informed consent to participate before taking part. In total, 2,206 participants answered and returned the questionnaires anonymously (response rate 73.5%). We excluded questionnaires that were answered by a person other than the participant (n=373), or who incompletely answered (n=230). The number of participants analyzed in the present study was 1,603 in total; 726 males (45.3%) and 877 females (54.7%). The effective response rate was 53.4%. The list of participants in the present study was constructed from the same database of our previous study9).
Measures
Basic attributes
Basic attributes included age, gender, household composition and subjective economic status. Age was classified into two categories: 65-74 years (‘early elderly’) and 75 years or older (‘late elderly’). Household composition was measured by choosing one of the following items: ‘single person’, ‘couple (age of spouse 65 years or older)’, ‘couple (age of spouse 64 years or younger)’, ‘living with one or more sons or daughters’, and ‘other’. The degree of subjective economic status was assessed using a five-point scale (1, ‘very good’; 2, ‘good’; 3, ‘fair’; 4, ‘poor’; and 5, ‘very poor’).
Health-related factors
Subjective health status, subjective happiness, current state/needs of assistance by others in daily life, frequency of participation in sports club activities such as exercise class for the elderly, and current/past health problems were assessed using the following questions, respectively: ‘How is your health now?’ (four-point scale: 1, ‘very good’; 2, ‘good’; 3, ‘bad’; and 4, ‘very bad’); ‘How happy are you now?’ (11-point scale: 1, ‘mostly unhappy’; to 11, ‘mostly happy’); ‘Do you need/receive daily assistance by others? (three-point scale: 1, ‘neither’; 2, ‘necessary, but do not receive any assistance’; 3, ‘necessary, and received’); ‘Please choose your current/past health problems’ (multiple answers allowed: nothing, hypertension, cerebrovascular disease, heart disease, diabetes, dyslipidemia, respiratory disease, gastrointestinal, liver and/or gallbladder disease, kidney and/or prostate disease, musculoskeletal disease, external injury, cancer, immunological and/or hematological disease, depression, dementia, Parkinson’s disease, eye disease, ear/nose/throat disease, and other); ‘How often do you participate in sports club activities?’ (six-point scale: 1, ‘over 4 times per week’; 2, ‘twice or 3 times per week’; 3, ‘once per week’; 4, ‘once to 3 times per month’; 5, ‘a few times per year’; 6, ‘no participation’).
Life-prolonging treatment
The outcome was the participant’s decision-making about treatment at the EOL stage, which was measured using the following question: ‘Do you prefer LPT at the EOL stage?’ (five-point scale: 1=‘definitely no’, 2=‘probably no’, 3=‘probably yes’, 4=‘definitely yes’, 5=‘undetermined’). Many of the previous studies on decision-making at the EOL have focused on whether the person would or would not prefer life-prolonging treatment4-11). However, the decision is not always easy to make, and many elderly people, especially those who are not in imminent danger of death, have not yet decided. Therefore, in this study, we will examine the decision-making of the elderly by three categories: ‘prefer’, ‘would not prefer’ and ‘undetermined’.
Statistical analysis
Prior to analysis, household composition was dichotomized: living alone for ‘single person’ and living with others for ‘couple (age of spouse was 65 years or older)’, ‘couple (age of spouse 64 years or younger)’, ‘living with one or more sons or daughters’, and ‘other’. The five degrees of subjective economic status were combined into three categories: poor for ‘very poor’ and ‘poor’, fair for ‘fair’, and good for ‘very good’ and ‘good’. The four degrees of subjective health status were dichotomized: bad for ‘very bad’ and ‘bad’, and good for ‘very good’ and ‘good’. As subjective happiness did not have a normal distribution, we set the cutoff at the 25th percentile in order to dichotomize the distribution: a ‘high’ group included participants with a subjective happiness rating of 7 or higher; and a ‘low’ group, consisting of participants with a rating of 6 or lower. The three degrees of assistance in daily life were dichotomized: yes for ’necessary, and received’ and no for ‘neither’ or ‘necessary, but do not receive any assistance’. The answers to the question of current/past health problems were classified as 0 or ≥1 based on the number of diseases chosen in the question. The six degrees of frequency of participation in sports club activities were dichotomized13): yes for ‘over four times a week’, ‘2 or 3 times a week’, ‘once a week’, ‘1 to 3 times a month’, ‘a few times a year’, and no for ‘no participation’. The five degrees of preference for LPT were classified into three categories: not prefer for ‘definitely no’ and ‘probably no’, prefer for ‘probably yes’ and ‘definitely yes’, and undetermined for ‘undetermined’.
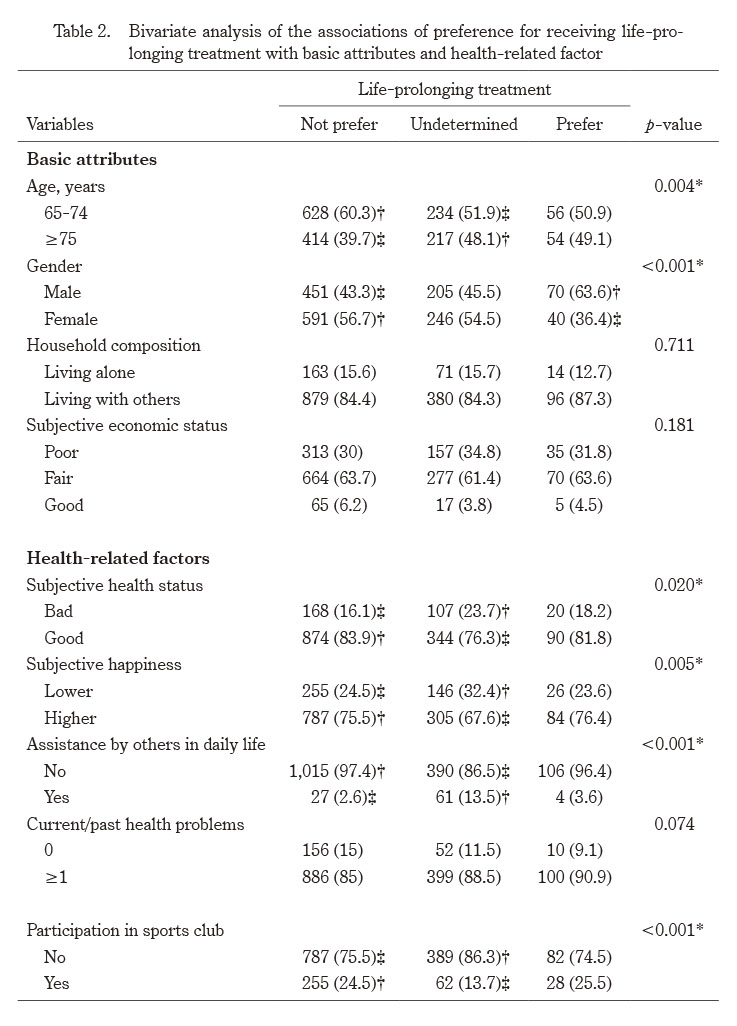
Statistical analyses were performed using SPSS statistics version 24 (IBM Corp., Armonk, NY, USA), and the participants’ characteristics were summarized using descriptive statistics. The bivariate associations between the above-mentioned factors and outcome variables were examined using a χ2 test, and then the statistical significance of the cells in the tables was analyzed using residual analysis.
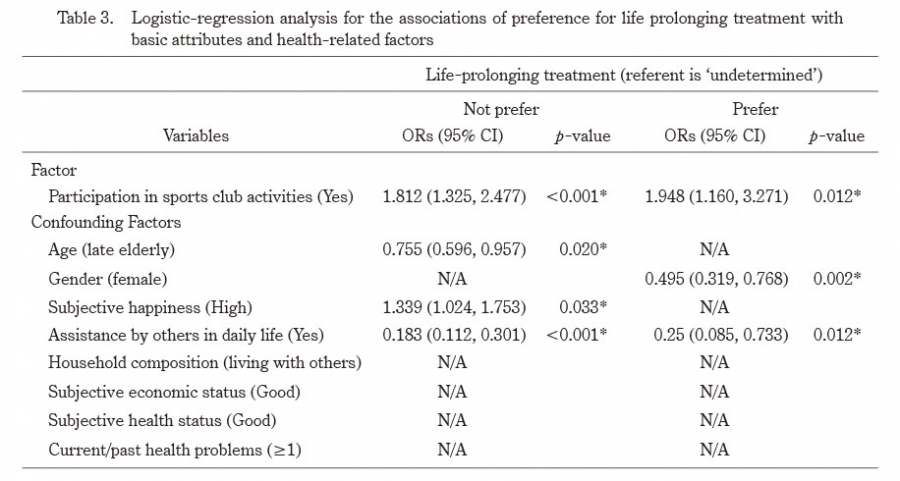
Multinomial logistic regression analysis models were prepared to estimate the association between preference for LPT and participation in sports club activities, adjusting for the following potential confounding factors: age, gender, household composition, subjective economic status, subjective health status, subjective happiness, current/past health problems and assistance by others. These were forced entry variables for analysis. Preference for LPT was employed as the dependent variable, setting the individuals who answered “undetermined” as the referent in order to examine whether participation in sports club activities is associated with an articulation of preference between LPT and non-treatment at the EOL stage. The independent variables that were significantly associated with preference for LPT with an odds ratio (OR) higher than 1 were considered to be promoting factors for expressing a clear decision on LPT, while those with ORs lower than 1 were considered to be inhibiting factors.
Variance inflation factor (VIF) was used to test for multicollinearity. The VIF values for age, gender, household composition, subjective economic status, subjective health status, subjective happiness, current/past health problems, need for assistance, and participation in sports club activities were 1.072, 1.024, 1.033, 1.139, 1.229, 1.160, 1.058, 1.105, and 1.037, respectively. The mean VIF of the model was less than 6, showing no collinearity.
P values below 0.05 were regarded as statistically significant. The OR and 95% confidence interval (CI) were calculated using regression analysis.
Ethics statement
This study was approved by the Ethics Committee of Fukushima Medical University (Application No. 29,047).