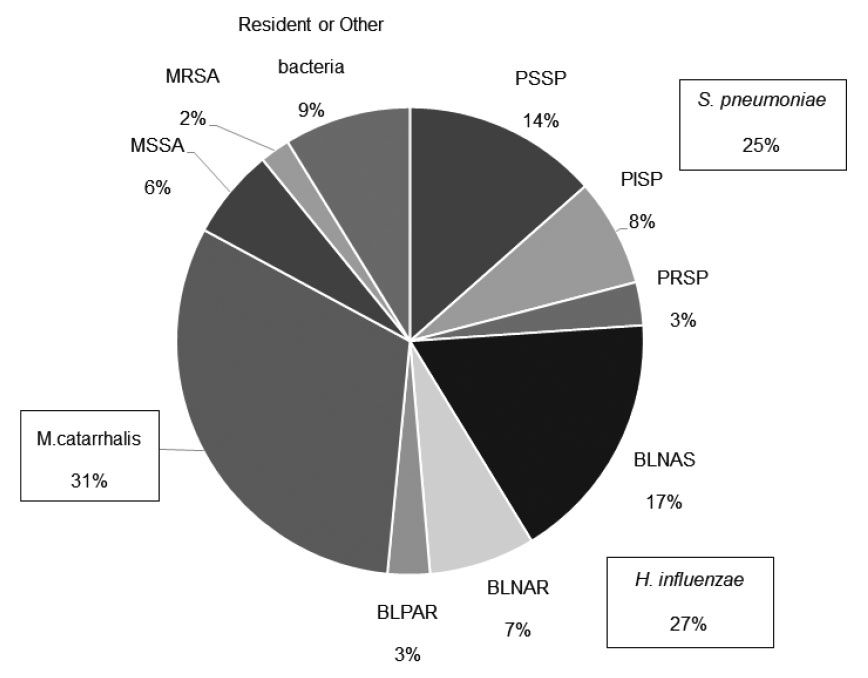
We investigated the nasopharyngeal culture on admission in children with lower respiratory tract infection and found that 99% (1,046 of 1,056) of these children had positive bacterial culture results;either S. pneumoniae, H. influenzae, or M. catarrhalis was isolated from 83% (874 of 1,046) of them.
Definitive methods for diagnosing the causative bacteria of pneumonia include isolation of bacteria from blood, pleural effusion, or lung puncture;however, these invasive methods were hardly suitable for the children in this study. In practice, transtracheal aspirations are routinely collected from intubated children and sputum from the pharynx is collected from non-intubated children for washed sputum culture6). As a practical matter, it is quite difficult to collect sputum from infants. The nasopharyngeal swab sample collection applied in this study has the advantage of noninvasive and reliable sampling. A matched case-control study demonstrated high concordance between nasopharyngeal and endotracheal aspirate samples or bronchoalveolar lavage fluid samples;thus, the authors presumed that nasopharyngeal microbiota can serve as a valid proxy for lower respiratory tract microbiota7). In contrast, another report indicated low concordance between isolates from nasopharyngeal swabs and bronchoalveolar fluid8). Because it is controversial whether the nasopharyngeal microbiota can reflect the lower respiratory tract microbiota, nasopharyngeal culture results should be collected as a reference finding;sputum and tracheal aspirate cultures should be performed as needed, especially in patients with severe respiratory infection.
S. pneumonia, H. influenzae, and M. catarrhalis, the three species most often isolated from the nasopharynx among patients in this study, are bacteria that colonize the nasopharynx early in life9);thus, it is unlikely that all isolated bacteria were pathogenic. However, the isolation rate of these bacteria is reportedly higher in children with upper respiratory tract infections than in healthy children10,11). Bacteria that proliferate in the upper respiratory tract after airway inflammation triggered by viral infection may also influence the development of lower respiratory tract inflammation by mechanisms such as entry into the lower respiratory tract and aspiration of airway secretions12,13). Accordingly, the nasopharyngeal microbiota is presumed to affect the onset of both upper and lower respiratory tract infections9). Furthermore, recent 16S RNA profiling-based analysis of the nasopharyngeal microbiota has revealed an association with subsequent wheezing14,15). Because of changes in environmental factors and their mutual relationship to the host, the nasopharyngeal microbiota presumably comprises both resident species and species involved in the development of lower respiratory tract infection7,16).
Regarding the involvement of S. aureus, our previous study showed that the number of children with isolates of the three major causative pathogens and the number of children with isolates of S. aureus or other bacteria were almost equal among older children (i.e., ≥4 years of age;data not shown). Multivariate analysis of factors associated with clinical severity between these two groups did not identify any statistically significant factors (data not shown). Thus, we concluded that the clinical impact of S. aureus or other bacteria on lower respiratory tract infection is low;additionally, the isolation rates of these bacteria were lower in patients under 6 years of age in the present study. Accordingly, we focused on children from whom at least one of the three major causative pathogens had been isolated.
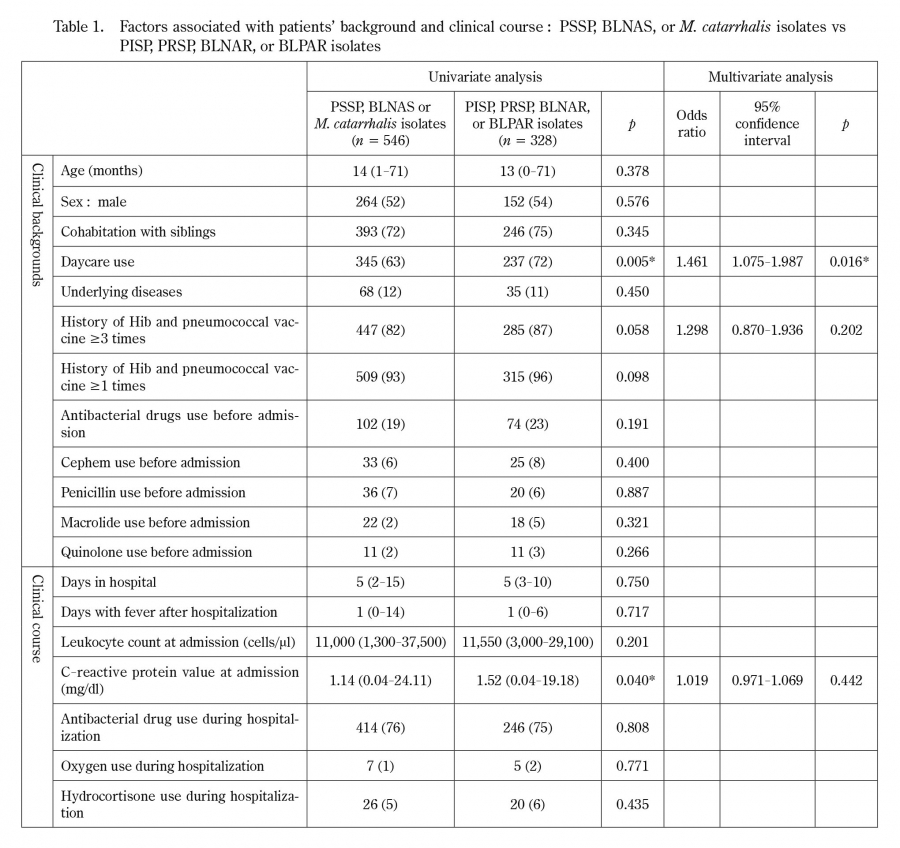
Further analysis in this study comprised examination of the clinical backgrounds and clinical course of patients in whom antibiotic-resistant bacteria were isolated from the nasopharynx. A multivariate analysis of all patients revealed that daycare use was the only significant predictor of antibiotic-resistant bacteria isolation. In the field of otolaryngology, it has been reported that children with recurrent otitis media frequently carry resistant bacteria17). However, children with resistant strains of bacteria do not necessarily exhibit refractory or recurrent otitis media;they are often asymptomatic18). Daycare facilities are densely populated and prone to droplet infection, and then may promote the spread of bacteria. Children recovering from upper respiratory tract infections are likely to be repeatedly infected by surrounding healthy carriers, leading to a high incidence of resistant strains17). The present study which investigated nasopharyngeal bacteria in preschool children, confirmed the association between daycare use and the transmission of antibiotic-resistant bacteria. These findings imply that daycare users should refrain from attending daycare facilities when they are symptomatic;daycare staff should perform thorough infection control measures.
In univariate analyses of clinical factors, the isolation of antibiotic-resistant strains was higher among patients who had received the Hib and pneumococcal vaccines, but this factor was not statistically significant in the multivariate analysis. This may be due to the high vaccination and hospital visit rates of patients using daycare facilities.
In this study, the isolation of antibiotic-resistant bacteria was not associated with factors related to the severity of lower respiratory tract infection (i.e., hospital stay length;period of post-hospitalization fever;or administration of antibacterial agents, oxygen, or hydrocortisone). For patients with lower respiratory tract infection who were treated with antibacterial agents, the need for such treatment was determined by comprehensively considering the clinical symptoms, laboratory findings, and clinical course. Piperacillin (2016-2017) or ampicillin (2018) was usually selected as the initial drug for treating lower respiratory tract infection;its selection was not based on an assumption of antibiotic-resistant bacteria. Because we found no association between the antibiotic resistance of nasopharyngeal bacteria and severity of lower respiratory tract infection, we recommend against using the results of nasopharyngeal culture as a basis for antibiotic selection or modification. For the initial selection of antibiotics to treat lower respiratory tract infection, our findings support the selection of narrow-range antibiotics without considering the possibility of antibiotic-resistant strains, except in patients with serious systemic infections that yield positive blood culture findings.
This study had a few limitations. First, virological examination of the patients was insufficient. Rapid antigen tests were performed in the patients according to the epidemic season, but not in all cases, and detection by polymerase chain reaction or other methods was not performed. Virus infection may be involved in the development of lower respiratory tract infection. In other reports, viruses and bacteria were simultaneously detected in the nasopharynx of children with lower respiratory tract infections19-21), and their interaction is assumed. Further studies are needed to evaluate the relationship between viral infections and resistant bacteria. Second, evaluations of the presence or absence of otitis media and sinusitis, blood culture, and antibody tests were not performed in some patients;moreover, some bacterial infections were insufficiently evaluated. Blood culture was performed for analysis of patients whose admission blood tests revealed a highly inflammatory reaction, but there were no patients with positive blood culture results who exhibited invasive bacterial infection.
This study suggests that the increased detection rate of resistant bacteria may be related to daycare use. In many instances, the isolation of such bacteria does not affect the severity of lower respiratory tract infection. Therefore, if antibacterial agents are used in the initial treatment of lower respiratory tract infection, narrow-range antibacterial agents should be selected in accordance with current guidelines for treatment of respiratory diseases in children.