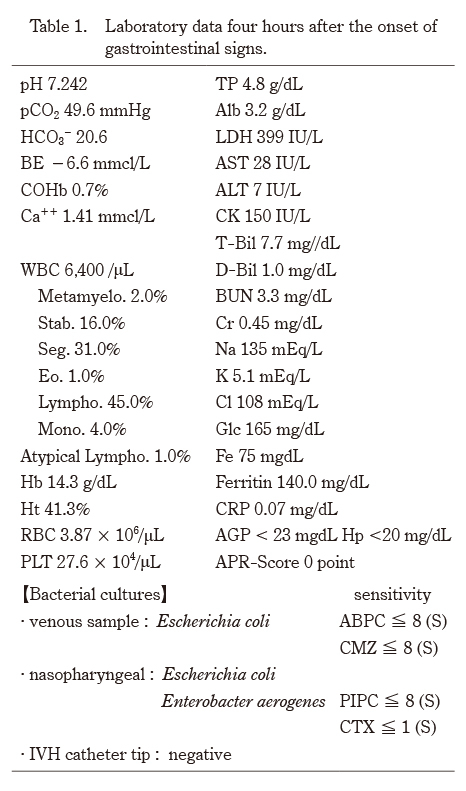
The transition of the APR was not significantly increased at 4 hours after the onset of gastrointestinal symptoms (Table 2), but CRP and AGP were remarkably increased at 12 hours after onset. Hp was below sensitivity from the beginning to end. CRP and AGP decreased once after the exchange transfusion but then increased to almost the previous value by 12 hours after the transfusion (Fig. 2).
IL-8 and IL-10 could not be measured at 5 hours after the onset because the sample volume was inadequate. However, the other four cytokines, (IL-1β, -6, TNFα, G-CSF), showed a significant increase at 5 hours after onset and then continued to increase. Although IL-1β and TNFα increased, the degree of increase of IL-6 and G-CSF was considerable compared to that of IL-1β and TNFα. IL-1β, TNFα, and IL-10 decreased once following the exchange transfusion, but all of them increased again to above their previous values in a short time. Rather, IL-6, IL-8 and G-CSF did not decrease.
With the exception of HMGB-1, there are no reference values for histone H3 and syndecan-1 in normal newborns4). However, due to the nature of these substances, it is hypothesized that the effect of perinatal hypoxic stress at 2 weeks after birth would be less than that of the acute period. Under this hypothesis, HMGB-1 and histone H3 were significantly increased 24 hours after onset5). Although syndecan-1 was also increased, it did not reach a level as high as its usual increase during adult sepsis, and it remained lower than the value seen in sepsis without disseminated intravascular coagulation6) (Fig. 3).
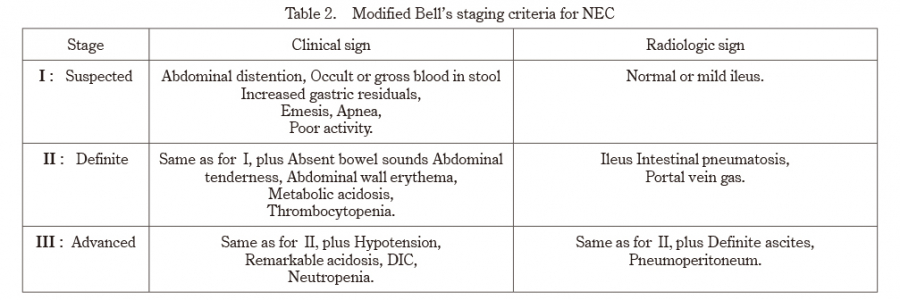
Table 2. Modified Bell’s staging criteria for NEC
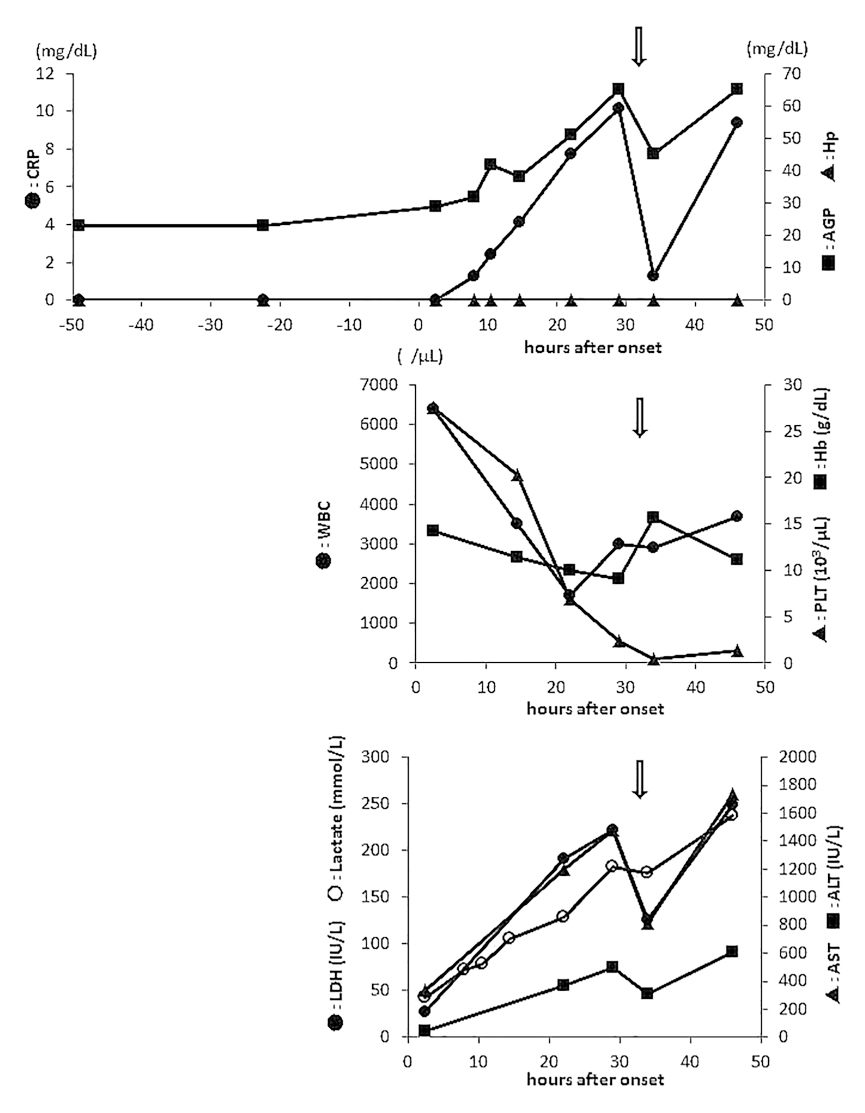
Fig. 2. Time course of acute phase reactants, peripheral blood cells, and releasing enzymes before and after onset:
Haptoglobin (Hp) remained negative from beginning to end. C-reactive protein (CRP) became positive 12 hours after the onset. The α1-acid glycoprotein (AGP) did not increase prior to CRP during feeding intolerance as has been previously reported. After onset, it increased slightly later than the increase in CRP. A decrease in these two acute phase proteins was seen once after exchange transfusion, but levels returned to the previous value in about half a day. White blood cell count and platelet count dropped sharply after onset. Hemoglobin did not decrease as much as the former two. Three of the releasing enzymes also increased after onset, did not increase to the same degree. Arrows mean blood exchange transfusion.
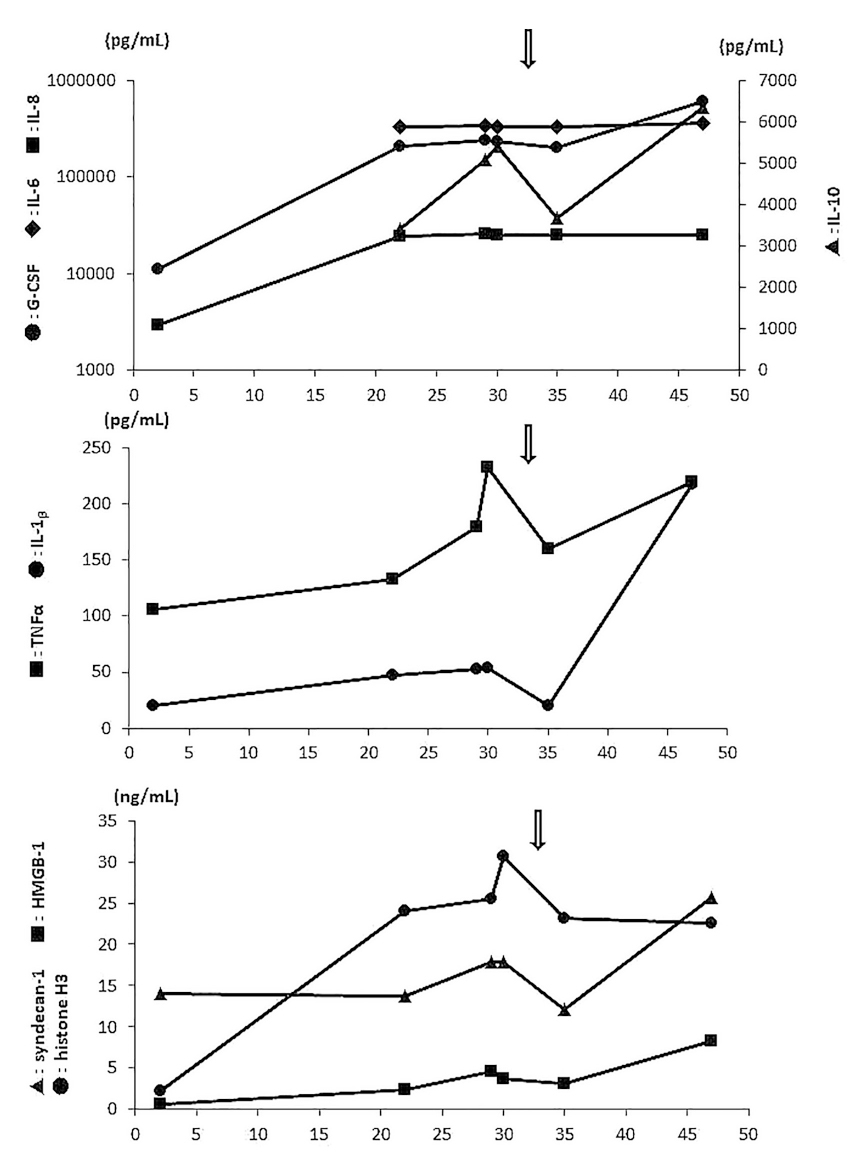
Fig. 3. Serial changes of cytokine profiles and the three cytotoxic markers after onset:
It can be seen that all six cytokines show high levels, and in particular, IL-6,-8,-10 and G-CSF have markedly elevated levels. Although these cytokines temporarily decreased after exchange transfusion, exacerbation exceeding the previous value was observed in about half a day. Considering the age of the newborn at onset, it is judged that the effect of ischemia-reperfusion injury at birth has disappeared. Based on this hypothesis, it is judged to be abnormal when these cytotoxic markers are present in the blood after onset. Considering adult reports, high mobility group box-1 (HMGB-1) and histone H3 are clearly elevated, but syndecan-1 is not significantly elevated. Serum syndecan-1 concentration in sepsis remains at a level that does not cause disseminated intravasclular coagulopathy. The arrows indicate blood exchange transfusion.