

Struma ovarii is a rare specialized form of ovarian teratoma that has been reported in approximately 3% of all ovarian teratomas1,2). It is sometimes difficult to differentiate from malignancy because it is a multicystic tumor with a solid component often accompanied by massive ascites3). Herein, we report a case of struma ovarii successfully treated with conservative laparoscopic surgery, even though malignancy was suspected preoperatively due to the presence of massive ascites and anelevated CA125 level.
The content of research paper
Struma ovarii with massive ascites mimicking ovarian carcinoma treated with conservative laparoscopic surgery: a case report
Riho Yazawa, Hiroyuki Yazawa, Kaoru Fukuda, Miki Ohara
Author information
-
Riho Yazawa
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
-
Hiroyuki Yazawa
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
-
Kaoru Fukuda
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
-
Miki Ohara
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
Introduction
Case
A 37-year-old nulliparous woman, never married and with no remarkable medical or family history, visited a local physician with a chief complaint of abdominal distention. She was suspected of having an ovarian tumor and referred to our department for evaluation and treatment. The patient had marked abdominal distention due to accumulation of massive ascites. No weight loss, tachycardia, abnormal ECG findings, or thyroid gland enlargement were noted. Contrast-enhanced computed tomography (CT) revealed bilateral ovarian tumors and accumulation of massive ascites, but no pleural effusion (Fig. 1). Blood tests showed anemia with hemoglobin of 6.2 g/dL. Level of the tumor marker CA125 was markedly elevated at 599.3 IU/mL. Other tumor markers were normal: CA19-9, 30.8 IU/mL; CEA, 0.5 ng/mL; and SCC, 1.4 ng/mL. On the day of admission, 1,000 mL of clear yellow ascites was collected by puncture for cytology; the cytological diagnosis was Class I, with no malignant cells. Seven days later, another 1,100 mL of ascites was obtained; the cytological diagnosis was Class II, with no malignant cells. On magnetic resonance imaging (MRI) (Fig. 2), the right ovarian tumor was found to be a dermoid cyst approximately 6 cm in diameter. The left ovarian tumor was over 10 cm in diameter, with partial fat suppression. It was also found to be a dermoid cyst but with a multicystic portion with low signal intensity on T1-weighted imaging (WI) and no fat components (Fig. 2A). It had high signal intensity on T2-WI (Fig. 2B, 2C). There was contrast enhancement within the cysts (Fig. 2D, 2E). The same portion had a slightly high signal on diffusion-WI and a low signal on apparent diffusion coefficient (ADC) mapping (Fig. 2F, 2G). On CT, the left ovarian tumor had an irregular thickened septum with contrast enhancement within the multicystic portion (Fig. 1C, 1E). There were no obvious findings of metastasis, lymph node swelling, or peritoneal dissemination. Based on the imaging findings described above, a malignant ovarian tumor was strongly suspected preoperatively. However, we also considered the possibility of a benign ovarian tumor, since two cytological examinations of ascites were negative. We decided to perform left adnexectomy and right ovarian cystectomy with intraoperative frozen section pathological examination. The surgery was performed laparoscopically, taking into consideration the patient’s wishes (Fig. 3).
Laparoscopic surgery revealed a 4,850 mL collection of clear, yellow ascites. The fluid was aspirated. The cytological examination was negative. The bilateral ovarian tumors had no adhesions (Fig. 3A). The right ovarian tumor was dermoid cyst-like. The left ovarian tumor was partly dermoid cyst-like, but included other irregularly shaped and multicystic masses with smooth surfaces (Fig. 3B, 3C). Laparoscopic left adnexectomy was performed (Fig. 3D) and the specimen was submitted for intraoperative pathological examination. The result suggested struma ovarii with no evidence of malignancy. There were no findings of dissemination on the peritoneum of the abdominal cavity. In addition, right ovarian cystectomy was performed (Fig. 3E, 3F).
The split surface of the left ovarian tumor was composed of a dermoid cyst and a multicystic tumor resembling a brown thyroid gland (Fig. 4B). Intraoperative rapid pathology results were indicative of struma ovarii with no evidence of malignancy (Fig. 4C). On postoperative pathological examination, the grossly teratoma-like area was a teratoma with a mixture of skin appendages and no immature portions. The grossly thyroid-like tumor area appeared to be a follicular adenoma or adenomatous goiter, with a background of healthy thyroid follicles and follicular epithelium forming small and large glandular lumens and substantial foci containing colloids (Fig. 4D-F). Immunostaining was performed to confirm struma ovarii and to differentiate it from thyroid carcinoid. The thyroid tumor marker TTF-1 was positive (Fig. 4G); chromogranin A and synaptophysin, markers of the endocrine system, were negative (Fig. 4H, 4I). These findings led to a diagnosis of teratoma, in which the left ovarian tumor contained thyroid follicular epithelium among the germinal components. The right ovarian tumor was a dermoid cyst with no immature components. Neither ovarian tumor had any malignant components. The diagnosis was mature teratoma with struma ovarii.
The postoperative course was uneventful. The patient was discharged on postoperative day 5. Blood tests showed a marked decrease in CA125 levels to within normal limits. No re-accumulation of ascites was found on transvaginal ultrasonography.
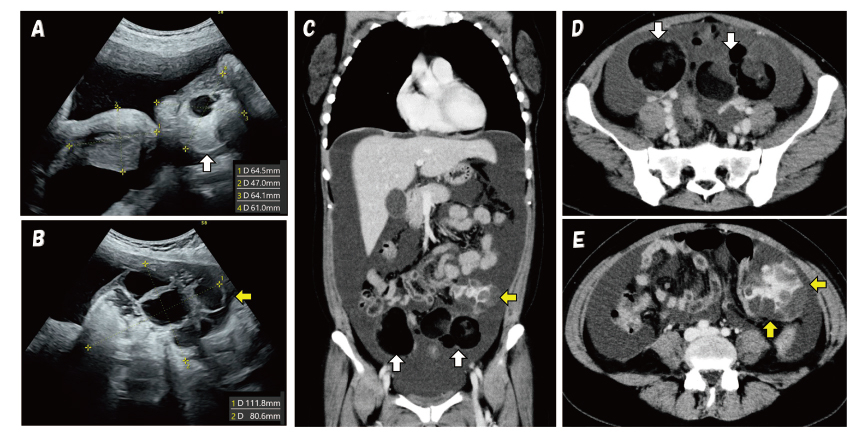
Fig. 1. Transabdominal ultrasonography and contrast-enhanced computed tomography (CT) findings
White arrows indicate dermoid cyst, yellow arrows indicate multicystic tumor (struma ovarii).
Transabdominal ultrasonography (A, B) revealed massive ascites, a uterus of normal size, a dermoid cyst of the rigth ovary (A) and a tumor with multicystic and solid components of the left ovary (B).
Similarly, CT (C-E) showed massive ascites, bilateral dermoid cysts, and a polycystic tumor of the left ovary with internal contrast-enhancing solid components (E). No metastases, disseminated lesions, or lymph node enlargement were observed on CT.
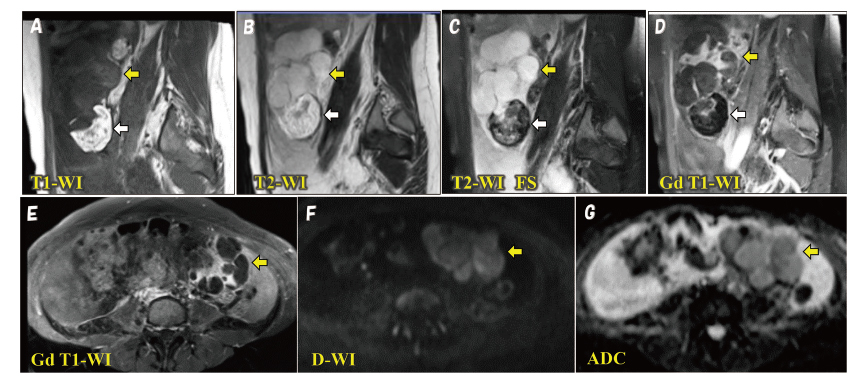
Fig. 2. Contrast-enhanced magnetic resonance imaging (MRI) findings
White arrows indicate dermoid cyst, yellow arrows indicate multicystic tumor (struma ovarii).
Contrast-enhanced MRI showed a multicystic portion of the left ovary (yellow arrow) with low signal intensity on T1 weighted imaging (WI) (A), and high signal intensity on T2-WI (B, C). The tumor had a thickened septum and a solid component with contrast enhancement inside (D,E). In addition, diffusion weighted imaging showed a slightly high signal signal inteisity (F) and low apparent diffusion coefficient (ADC) values (G).
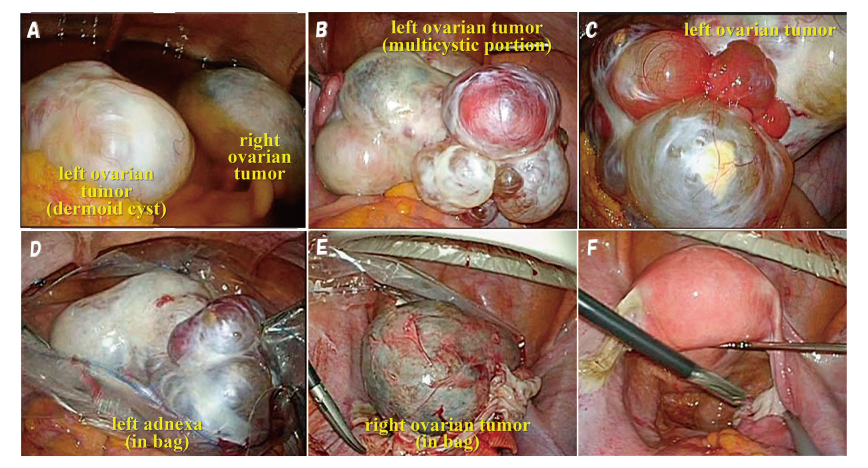
Fig. 3. Findings during laparoscopic surgery
The abdominal cavity was observed after aspiration of approximately 3,400 mL of ascites (A). Bilateral ovarian tumors were observed: a dermoid cyst on the right ovary (A) and a dermoid cyst plus a multicystic tumor on the left ovary (B,C). Left adnexectomy was performed (D) and the specimen was submitted for intraoperative frozen section pathological examination. Right cystectomy was also performed (E). The operation was completed (F).
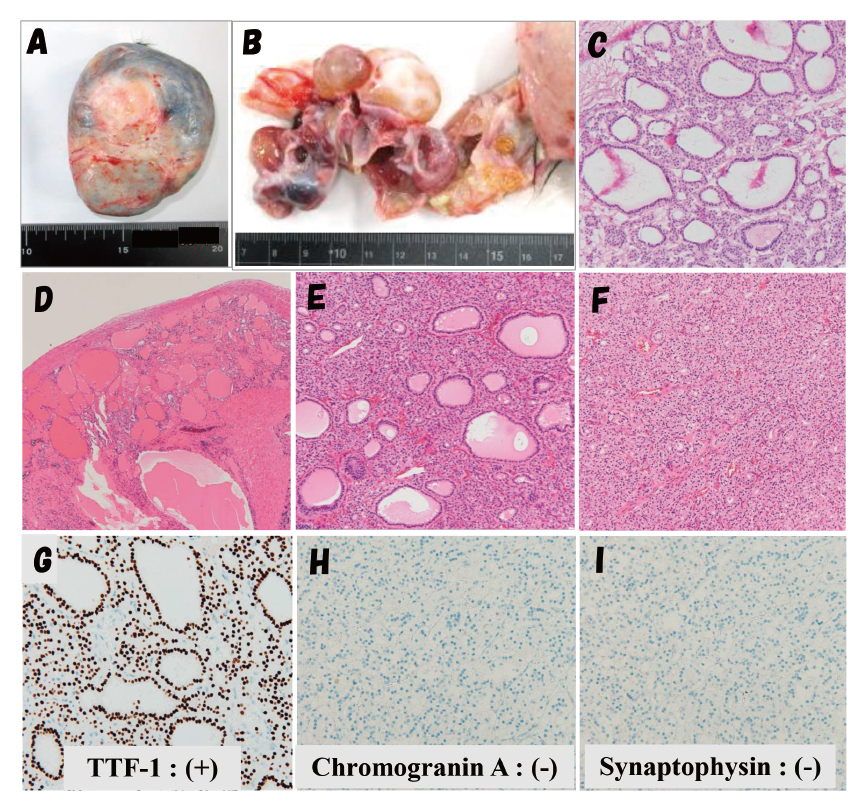
Fig. 4. Histopathological findings
The right ovarian tumor was a dermoid cyst (A). A part of the left ovarian tumor was a dermoid cyst. Another part was a multicystic tumor (B). The multicystic portion containing jelly-like viscous contents had an irregular, thickened septum and solid components (B). Rapid pathological examination revealed numerous small and large adenoidal ducts containing a pale acidic colloid-like internal fluid, suggesting a thyroid follicular adenoma derived from struma ovarii, with no evidence of malignancy (C). On postoperative pathology, the same area had a background of healthy thyroid follicles (D). The pale follicular epithelium of the follicles formed small and large glandular ducts containing colloids, similar to findings in follicular adenoma or adenomatoid goiter (E). The diagnosis was struma ovarii (D-F). Immunohistochemistry results showed that the thyroid tumor marker TTF-1 was positive (G). Chromogranin A (H) and synaptophysin (I) were negative, which signified no thyroid carcinoid component.
Discussion
Struma ovarii is a rare specialized form of ovarian teratoma that has been reported to comprise 0.5-1.0% of all ovarian tumors and approximately 3% of all ovarian teratomas1,2). It is defined as an ovarian teratoma that is composed predominantly of mature thyroid tissue (>50% of the ovarian mass overall) or forms a macroscopically recognisable component of mature cystic teratoma1,3). It usually presents as an asymptomatic pelvic mass. Struma ovarii is difficult to diagnose prior to surgery, although it may present with hyperthyroidism in approximately 5% of cases4,5). Malignant struma ovarii accounts for approximately 5-10% of struma ovarii that can be histologically identified as differentiated thyroid carcinoma6,7).
It is challenging to diagnose struma ovarii with preoperative imaging alone. Although it is often difficult to differentiate struma ovarii from ovarian carcinoma, ultrasonography, MRI, and CT can be useful for diagnosis. On ultrasonography, typical cases consist of multicystic tumors with an irregular septum and irregular echogenic solid components inside. Color Doppler findings can vary from no to abundant blood flow, depending on the case. A characteristic finding is the presence of circumscribed, round, and solid areas with smooth contours that correspond to colloid-rich thyroid tissue; it has been named the “struma pearl”8-10). On MRI, it has been reported that multicystic tumors with solid components often have high signal intensity on T1-WI, while the cystic part has various signal intensities on T2-WI depending on the viscosity of the fluid. The solid components often have moderate to high signal intensity on T1-WI8,11). On CT, enhancement of the septum or solid component is variable, depending on the contents of the thyroid tissue8,11). In practice, it is not very easy to diagnose struma ovarii preoperatively based on the imaging findings described above. In most cases, a definitive diagnosis is reached through postoperative pathological examination.
In our patient, the left ovarian tumor was a multicystic tumor with an irregular thickened septum and a solid component, mimicking ovarian carcinoma. We could not identify any “struma pearl” on ultrasonography (Fig. 1B). MRI showed slightly high signal intensity on T2-WI and low signal intensity on T1-WI, with a thickened septum and a solid component with contrast enhancement and mild diffusion restriction on D-WI (Fig. 2).
Although struma ovarii is generally a benign tumor, 15-20% of cases present with ascites. Rarely, it is accompanied by ascites and pleural effusion, which is called pseudo-Meigs’ syndrome8). Meigs' syndrome is a condition in which substantial benign solid ovarian tumors such as fibromas and thecomas are associated with ascites and pleural effusion; it was first described by Meigs in 195412). On the other hand, ovarian tumors other than fibromas and thecomas (i.e., cystic ovarian tumors, teratomas, or uterine leiomyomas) with ascites and pleural effusion are called pseudo-Meigs’ syndrome13). The mechanism of ascites accumulation in Meigs’ or pseudo-Meigs’ syndrome is uncertain, but Amant et al. speculate that it may be due to peritoneal irritation by the tumor, lymphatic obstruction, production of toxins and inflammatory products, decreased venous return, and hypoalbuminemia13). The dye test suggests that mechanical transfer of ascites through a diaphragmatic opening is a factor in pleural effusion13).
To date, some cases of struma ovarii with massive ascites or pseudo-Meigs’ syndrome have been reported and reviewed. Fujiwara et al. reviewed struma ovarii with elevated serum CA125 levels and massive ascites (13 patients) or pseudo-Meigs’ syndrome (14 patients)8). The age of onset among the 27 patients was in the 30s for 1 patient, in the 40s for 3 patients, in the 50s for 11 patients, and in the 60s or older for 12 patients, suggesting that older patients were more frequently affected than with typical mature teratoma. The preoperative diagnosis in 24 of the 27 patients was suspected ovarian carcinoma; 20 patients underwent intraoperative diagnosis with frozen section examination. Of these, 17 were diagnosed with struma ovarii. In terms of surgical technique, total abdominal hysterectomy (TAH) + bilateral salpingo-oophorectomy (BSO) was performed in 8 patients, TAH + BSO + omentectomy with or without lymph node biopsy or dissection in 11 patients, laparoscopic adnexectomy after preoperative chemotherapy in 1 patient, and, as in our case, laparoscopic adnexectomy alone with intraoperative pathological diagnosis in 1 patient8). Similarly, Jin et al. reviewed 11 cases of struma ovarii with elevated serum CA125 levels as well as ascites, pleural effusion, or both14). The age of onset was in the 40s for 2 patients, in the 50s for 4 patients, and in the 60s or older for 5 patients; 8 patients were postmenopausal. Four patients underwent TAH + BSO, five underwent TAH + BSO + omentectomy with or without lymph node sampling, and two underwent adnexectomy. The mean tumor diameter was 10 cm. Furthermore, they reported that all but one of the 10 patients were suspected of having a malignant ovarian tumor preoperatively. As mentioned above, in many cases of struma ovarii, ovarian carcinoma is suspected preoperatively and diagnosed with intraoperative pathological examination involving frozen section. There are also scattered cases of unnecessary extensive surgery based on incorrect diagnosis8,14). Fujiwara et al. reported that, in addition to conventional imaging examination, thyroid scintigraphy and positron emission tomography (PET)-CT are useful for differentiating between ovarian cancer and struma ovarii8).
In our patient, multicystic and solid tumors of the left ovary with massive ascites were found and laboratory data showed elevated serum CA125 levels and severe anemia. At the time of initial examination, hemorrhagic ascites due to ovarian carcinoma and peritonitis carcinomatosa (carcinomatous peritonitis) were strongly suspected. After hospitalization, two ascites punctures revealed clear yellow ascites, not bloody ascites. Cytology was negative both times and no disseminated lesions were observed on detailed imaging. Thus, we considered that the patient might have a benign ovarian tumor. During preoperative informed consent, the possibility of a malignant or benign tumor was fully explained. As a result, we decided to perform laparoscopic left adnexectomy with an intraoperative frozen section pathological examination, taking into consideration the patient’s wishes, although she did not wish to undergo fertility preservation surgery if the tumor was malignant. If intraoperative pathological diagnosis with frozen section showed malignant findings, we planned to perform open radical abdominal surgery (TAH + BSO + pelvic and para-aortic lymphadenectomy + omentectomy). Since intraoperative pathological diagnosis suspected struma ovarii with no evidence of malignancy, the operation was completed with removal of the left adnexa and right ovarian cystectomy. The pathological diagnosis of the permanent specimen was mature cystic teratoma of the right ovary and mature cystic teratoma and struma ovarii of the left ovary with no malignancy. The patient is progressing well without any re-accumulation of ascites and blood tests showed a decrease in CA125 levels within normal limits.
Conclusion
Struma ovarii can include a multicystic tumor with solid components. Preoperative differentiation from malignant ovarian carcinoma can be problematic. Furthermore, when a patient presents with accumulation of massive ascites and an elevated CA125 level, as in our case, a malignant ovarian tumor is strongly suspected. The literature describes unnecessary and excessive surgery in some cases. Because benign struma ovarii is a disease that can be treated with only surgical resection of the tumors, conservative surgery (cystectomy or adenectomy) should be chosen when it is accurately diagnosed (e.g., with intraoperative or postoperative pathological examination). In particular for patients who wish to preserve their fertility, laparoscopic conservative surgery can be indicated.
Conflict of interest
The authors have no conflicts of interest to declare.
Patient consent
We obtained informed consent from the patient for the publication of this work.