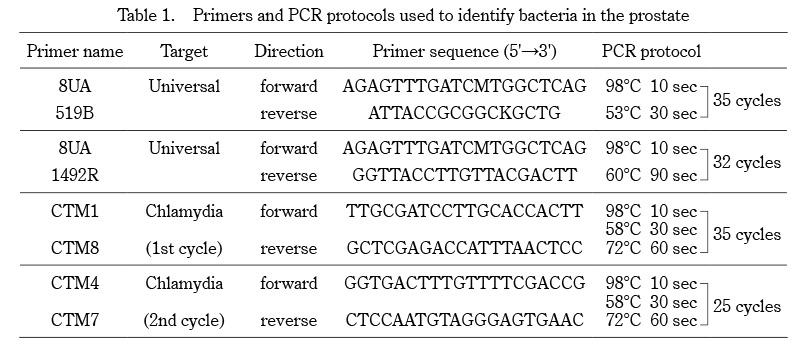
Prostate biopsies were taken from 97 patients. The presence or absence of bacteria was assessed by sequencing as described. The identification of 16S sequences indicated the presence of bacteria in the prostates of 7 patients (7.2%). Five genera of bacteria were identified by their 16S sequences; Streptococcus mitis (1/97, 1.0%), Staphylococcus haemolyticus (1/97, 1.0%), Chlamydia trachomatis (3/97, 3.1%), Cutibacterium acnes (1/97, 1.0%), and Acidovorax sp (1/97, 1.0%) (Figure 1). One bacterial species was detected in each patient, and no patient had more than one bacterial species.
To clarify associations between patient background and the presence of bacteria in prostate tissue, we compared age, height, body weight, presence of comorbidities such as hypertension and diabetes, PSA, and prostate volume between bacteria-present and -absent groups. There were no statistically significant differences in patient characteristics between the two groups (Table 2).
Differences in histological findings between the bacteria-present and -absent groups were evaluated. Of the patients with bacteria in the prostate, only one had histological evidence of malignancy, with no significant difference in the proportion of patients with prostate cancer between the two groups (p = 0.10) (Table 3). Moreover, there was no significant difference in ISUP Grade between the two groups (p = 0.12).
Next, we compared the stroma-to-gland ratio in prostate biopsies without malignant findings (n = 54) between the two groups. The stroma-to-gland ratio in the bacteria-present group was lower than that in the bacteria–absent group, suggesting that glandular components were predominant in bacteria-present group (p < 0.01) (Figure 2). In addition, histological evaluation revealed that prostate glands in the bacteria-absent group had a uniform monolayer arrangement. On the other hand, prostate glands in the bacteria-present group had ductal structures longer in shape, with irregularities in their nuclear arrangement, suggesting that glandular epithelial hyperplasia had developed in the bacteria-present group.
We also evaluated the association between the presence of bacteria in prostate tissues and LUTS. There were no significant differences in LUTS evaluated by IPSS, QOL score, or OABSS between the two groups. In addition, MFR, VV, and PVR were examined to determine the relationship between the presence of bacteria in prostate tissues and lower urinary tract function. Again, no significant differences emerged between the two groups. (MFR, p = 0.630; VV, p = 0.710; PVR, p = 0.730) (Table 4).
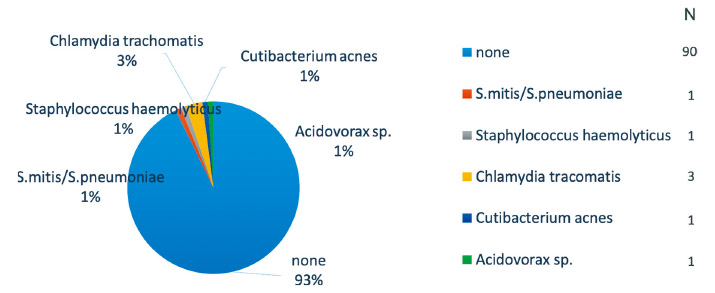
Fig. 1. Bacteria in prostate tissues
Bacteria were present in the prostates of seven patients (7.2%). Chlamydia trachomatis was the most common (3/97, 3.1%), followed by Streptcoccus mitis (1/97, 1.0%), Staphylococcus haemolyticus (1/97, 1.0%), Chlamydia trachomatis, Cutibacterium acnes (1/97, 1.0%), and Acidovorax sp. (1/97, 1.0%).
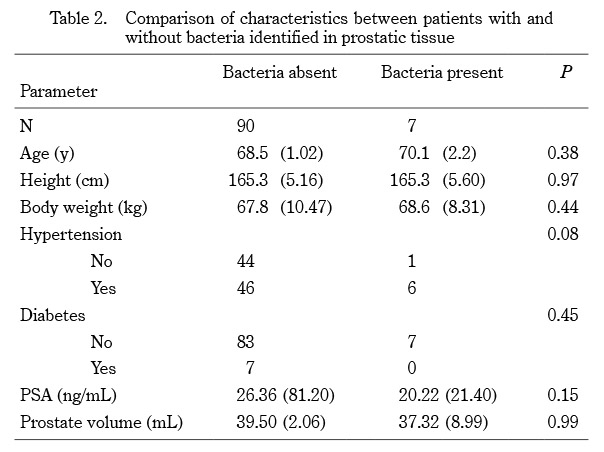
Table 2. Comparison of characteristics between patients with and without bacteria identified in prostatic tissue
Mean (SD: standard deviation)
PSA, prostate-specific antigen. Statistical significance threshold, P < 0.05.
Table 3. Association between the presence of bacteria in prostate tissue and prostate cancer
ISUP, International Society of Urological Pathology.
Statistical significance threshold, P < 0.05.
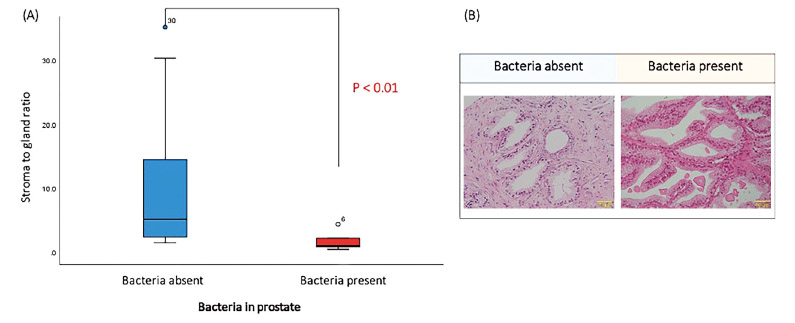
Fig. 2. Stroma-to-gland ratio and the presence or absence of bacteria in prostate tissues
The stroma-to-gland ratio in prostate tissues without malignant findings (n = 54) was compared in cases without bacteria (n = 48) and with bacteria (n = 6). The stroma-to-gland ratio in cases with bacteria was significantly lower than that in cases without bacteria. This suggests an association with an increase in glandular duct structure (A). Representative cases are shown in (B) (200×).
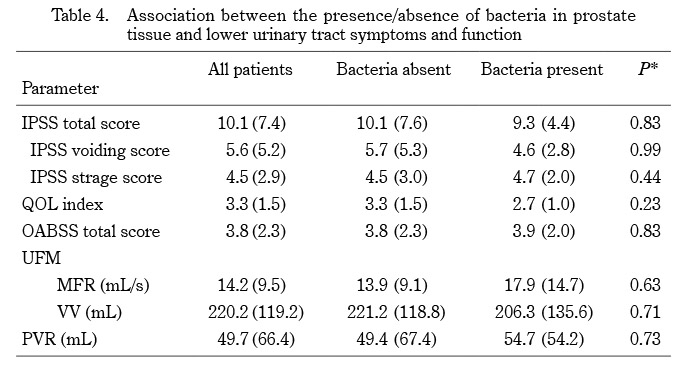
Table 4. Association between the presence/absence of bacteria in prostate tissue and lower urinary tract symptoms and function
IPSS, International Prostate Symptom Score; QOL, Quality of Life; OABSS, Overactive Bladder Symptom Score; UFM, Uroflowmetry; MFR, maximum flow rate; VV, voided volume; PVR, post-voided residual urine volume.
Mean (SD: standard deviation). Statistical significance threshold, P < 0.05.
*Bacteria-absent group vs Bacteria-present group