

Polypoid endometriosis is a rare variant of endometriosis characterized by the development of polypoid masses from ovarian or extra-ovarian endometriotic lesions. It is a benign disease with histological features resembling those of endometrial polyps, but can be difficult to distinguish from malignancy preoperatively or even intraoperatively. We report a case of polypoid endometriosis that grew rapidly and was strongly suspected to represent advanced ovarian carcinoma.
The content of research paper
A case of polypoid endometriosis mimicking advanced ovarian carcinoma with rapid growth, invasion, and dissemination
Hiroyuki Yazawa, Riho Yazawa, Kaoru Fukuda, Miki Ohara
Author information
-
Hiroyuki Yazawa
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
-
Riho Yazawa
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
-
Kaoru Fukuda
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
-
Miki Ohara
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
Introduction
Case
A 46-year-old nulliparous woman was referred to our department with symptoms of hypermenorrhea and severe anemia, with a diagnosis of multiple uterine fibroids and left ovarian tumor. Her initial blood tests showed hemoglobin and CA125 levels of 6.6 g/dL and 113 IU/mL, respectively, and contrast-enhanced magnetic resonance imaging (CE-MRI) showed a subserosal myoma measuring 6 cm × 14 cm and a left ovarian endometrial cyst. After administration of a gonadotropin-releasing hormone (GnRH) agonist (leuprorelin, 1.88 μg) for 4 months, laparoscopic subserosal myomectomy and left adnexectomy were performed (Figure 1. A, B). The pathological diagnoses were leiomyoma and endometrial cyst. Surgical findings showed adhesions in the rectum, sigmoid colon, and posterior uterus in the pouch of Douglas, and firm adhesions in the right adnexa and ileocecal area (Figure 1. C). The adhesions were detached to the greatest extent possible, and the right ovary was found to be almost normal (Figure 1. D). Subsequent imaging revealed no significant changes through 7 months postoperatively, but rapid enlargement of the right ovarian tumor was detected 11 months postoperatively. CE-MRI (Figure 2) and contrast-enhanced computed tomography (CE-CT) showed a lump in the right adnexa and ileum, as well as masses in the sigmoid colon and right upper abdominal wall. Fluorodeoxyglucose (FDG) PET-CT showed increased uptake in the abdominal wall tumor (Figure 3), and intestinal invasion and peritoneal dissemination of ovarian cancer were strongly suspected. During this period, the patient developed intestinal obstruction and was urgently admitted to the Department of Gastroenterology. A colonoscopy showed marked stenosis of the intestinal tract due to numerous submucosal lesions in the rectum and sigmoid colon, and a stent was inserted in the area (Figure 4. A, B, C). Immunohistochemical staining of tumor biopsy samples from the sigmoid colon were CK7(+), CK20(−), CDX2(−), and HNF4α(−). The tumor was suspected to be of extraintestinal origin and was estrogen receptor positive, which suggested intestinal endometriosis (Figure 4. E, F). As treatment, exploratory laparotomy was performed to biopsy the tumor, since primary debulking surgery was deemed to be difficult. The right adnexal tumor and ileal tumor formed a lump in the pelvic cavity, and a large omental tumor was present just below the upper abdominal wall; thus, removal of the omental tumor and biopsy of the right adnexal tumor were performed. Intraoperative rapid pathological examination revealed disseminated endometriosis with no evidence of malignancy, and assessment of a permanent specimen resulted in a diagnosis of polypoid endometriosis (Figure 5. Upper row; A, B, C).
The patient was started on a GnRH antagonist (relugolix; 2 mg/day) after surgery. Three months later the right adnexal tumor had shrunk markedly to 32 mm × 36 mm (Figure 6), but there was no significant change in the ileocecal mass. The patient underwent a third operation consisting of right adnexectomy and ileocecectomy. The uterus and sigmoid colon could not be removed, because they were firmly adhered to each other and consent for a contingency colostomy could not be obtained preoperatively. Postoperative pathology showed that the tumor invading the cecal mucosa from the ovary was polypoid endometriosis with no malignant findings (pPM0, pDM0, pRM0, negative margins) (Figure 5. Lower row; D, E, F). A low-grade appendiceal mucinous tumor (pT3, SS, Ly0, V0, negative margins) was also found incidentally.
The patient has been under observation for more than 1 year since the latest surgery and has been asymptomatic. The stent inserted in the sigmoid colon was ejected spontaneously. Colonoscopy performed 6 months after the final surgery showed that the polypoid tumor of the sigmoid colon was still present but was smaller in size, and that intestinal stenosis had markedly improved (no abnormalities were observed in the ileocecal region) (Figure 7). CA125 and CA199 levels remained within the normal range, and the blood estradiol level remained <10 ng/ml.
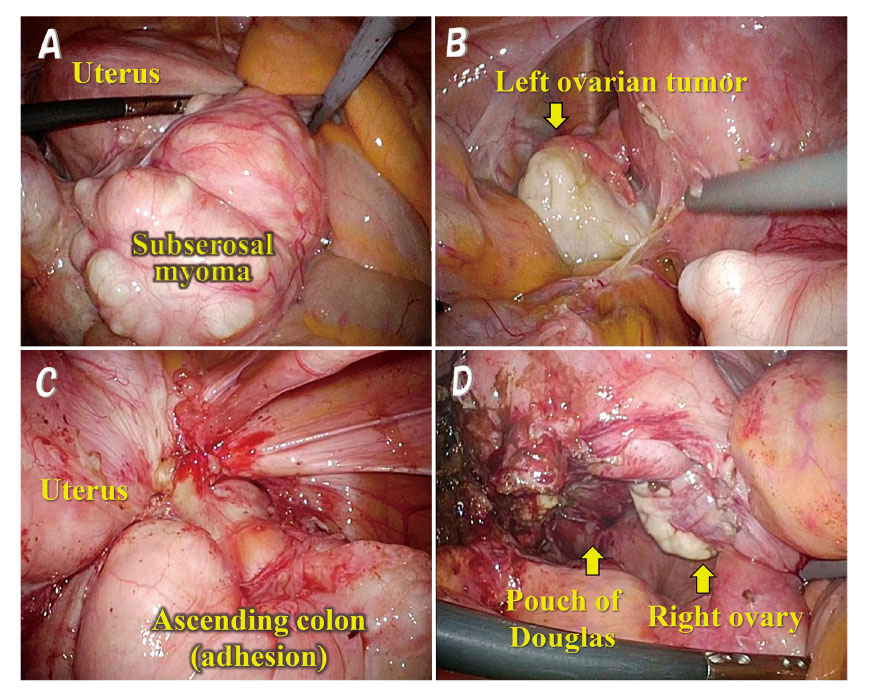
Fig. 1. Findings during first laparoscopic surgery.
Laparoscopic subserosal myomectomy (A) and left adnexectomy (endometrial cyst) (B) were performed. Surgical findings showed adhesions in the rectum, sigmoid colon, and posterior wall of the uterus in the pouch of Douglas, and firm adhesions in the right adnexa and ileocecal area (C). When the adhesions were detached, the right ovary was found to be almost normal (D).
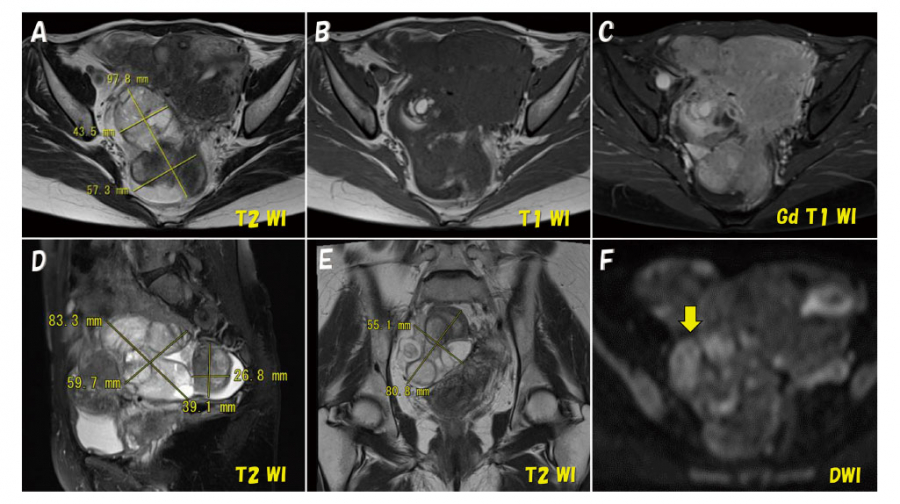
Fig. 2. Findings of CE-MRI of the right ovarian tumor performed about 1 year after the first laparoscopic surgery.
CE-MRI showed a lump in the right adnexa and ileocecal area, with a size of about 6 cm × 10 cm.
Axial T2-weighted image showing a hyperintense mass (A). Axial T1-weighted image showing isointensity with some hyperintense masses (B). Axial T1-weighted image with gadolinium contrast showing mild tumor enhancement (C). Sagittal T2-weighted image (D). Coronal T2-weighted image (E). Diffusion-weighted image showing slightly high signal intensity (arrow) (F).
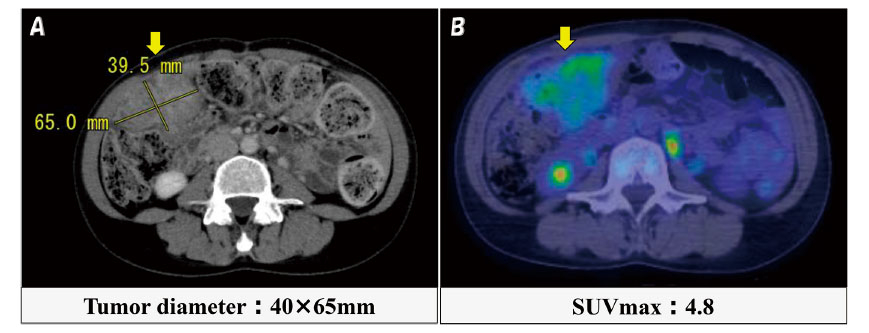
Fig. 3. Findings of PET-CT of the omental tumor.
PET-CT showed faint FDG accumulation in the omental tumor in the right upper abdominal wall (arrow) (A, B).
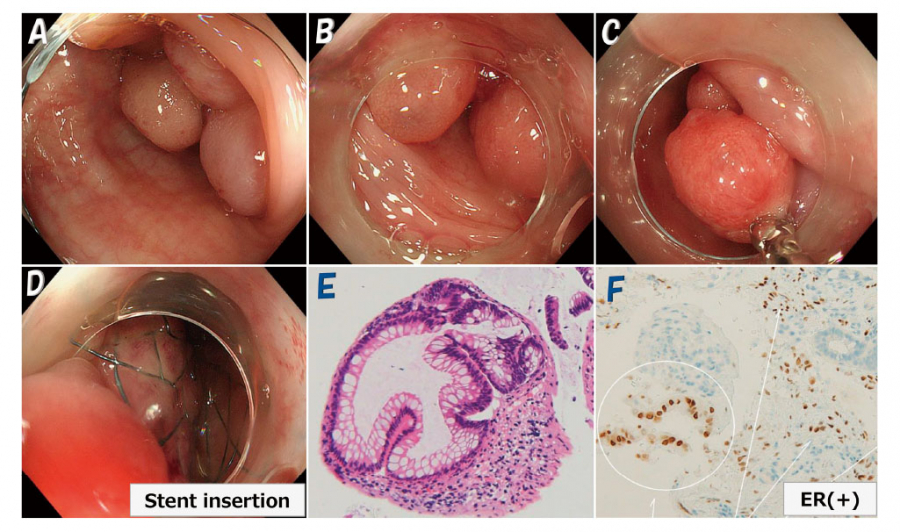
Fig. 4. Findings of colonoscopy performed before the second surgery and pathologic examination of a biopsy specimen.
Colonoscopy showed marked stenosis of the intestinal tract due to multiple submucosal polypoid lesions in the sigmoid colon (A, B, C), and a stent was inserted in the area (D). Pathological examination of a biopsy specimen was suggestive of intestinal endometriosis, because the endometrial grand-like atypical gland were ER-positive (E, F).
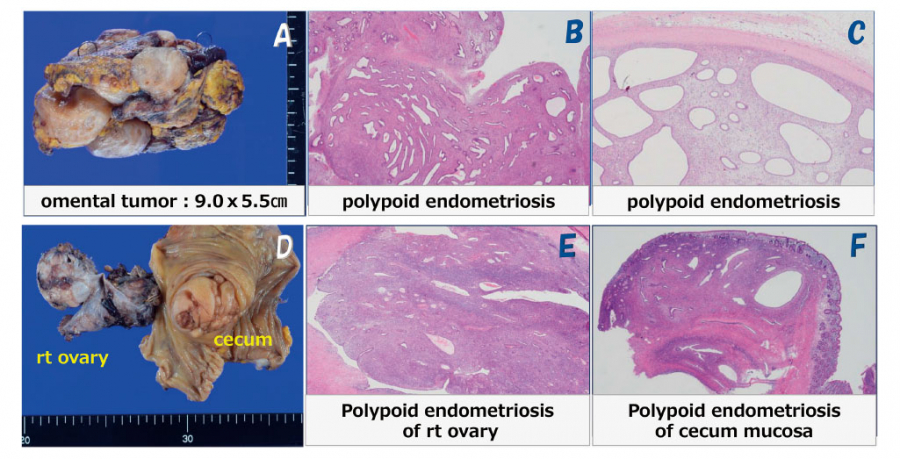
Fig. 5. Histopathological findings of removed organs from the second and third surgeries.
Upper row (A, B, C):In the second surgery, removal of the omental tumor was performed and a permanent specimen was pathologically diagnosed as polypoid endometriosis with no malignancy.
Lower row (D, E, F):In the third surgery, right adnexectomy and ileocecectomy were performed and pathologically diagnosed as polypoid endometriosis with no malignancy.
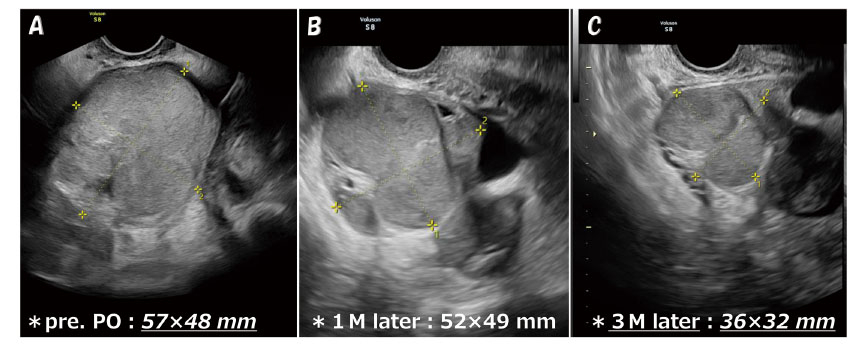
Fig. 6. Findings of transvaginal ultrasonography before and after administration of a GnRH antagonist.
The size of the right adnexal tumor markedly decreased after the patient was started on a GnRH antagonist (relugolix;2 mg/day) following the second surgery. The right adnexal tumor measured 57 mm × 48 mm pre-administration (A), 52 mm × 49 mm 1 month later (B), and 32 mm × 36 mm 3 months later (C).
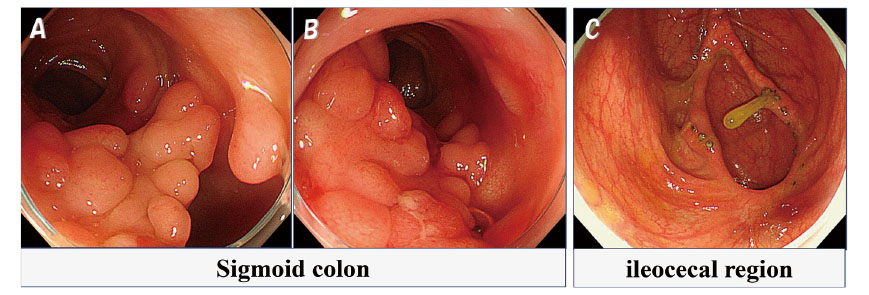
Fig. 7. Findings of colonoscopy performed 6 months after the third surgery.
Colonoscopy showed that the polypoid tumor of the sigmoid colon was still present but had decreased in size, and that intestinal stenosis had markedly improved (A, B). No abnormalities were observed in the ileocecal region (C).
Discussion
Polypoid endometriosis is a rare form of endometriosis characterized by the development of polypoid ovarian or extra-ovarian endometriotic lesions. It is a benign disease with a histology often resembling endometrial polyps, with endometrioid-type glands and stromal structures and often abundant fibrous stroma with thick-walled vessels1). It was first described by Mostoufizdeh and Scully in 19802). Polypoid endometriosis is most prevalent in women aged 40-50 years, thus occurring slightly later than usual endometriosis, often even after menopause. The ovaries and colon (rectum and sigmoid colon) are the most common sites of onset, but lesions can arise in a variety of locations, including the uterus, bladder, ureter, peritoneum, and omentum3,4). Polypoid endometriosis is often difficult to distinguish from malignancies, both preoperatively and intraoperatively, because of the multiple, solid, rapidly growing lesions and their frequent recurrence5).
In 2004, Parker et al. published a detailed report of 24 polypoid endometriosis cases6), with age of onset ranging from 23 to 78 years (mean 52.2 years, median 55 years), and 60% over age 50. The most common sites of onset were the large intestine and mesentery (7 cases), followed by the ovary (6 cases), uterine serosa (4 cases), vaginal mucosa (4 cases), ureter (3 cases), cervix (2 cases), fallopian tubes (2 cases), and omentum (2 cases). There were multiple lesions in 7 cases and single lesions in 17 cases, and the lesions arose from ovarian or extra-ovarian endometrial cysts in 5 cases. The presenting manifestations included pelvic tumor (14 cases), vaginal polypoid mass (4 cases), large bowel obstruction (3 cases), hematuria due to ureteral obstruction, adrenal mass, and ovarian cyst (1 case each). In terms of symptoms, abdominal pain (4 cases) and genital bleeding (vaginal bleeding, 4 cases) were frequent, while dysmenorrhea, chronic pelvic pain, dyspareunia, and infertility, which are common symptoms of endometriosis, were rarely reported. Of the 17 patients who could be followed up after surgery, 16 survived (only one of whom had residual endometriosis) and one died of other causes; therefore, the prognosis was good. Prior to the development of polypoid endometriosis, 7 of the 24 patients received unopposed estrogen and 4 were treated with combined estrogen-progestin therapy (8 of these 14 patients were over 50 years of age and 3 were under 50 years of age), suggesting an association between exogenous hormones or hyperestrogenism and the development of polypoid endometriosis. There was one case of ovarian thecoma; in this case, hyperestrogenism due to an estrogen-producing tumor was suggested as a possible trigger.
There have been other case reports in which polypoid endometriosis was presumably caused by postmenopausal hormone replacement therapy (age 60)6), treatment of a young endometriosis patient with oral contraceptives (age 30)7), GnRH analogue treatment for recurrent severe endometriosis8), and postoperative tamoxifen administration for breast cancer9-12). Although tamoxifen is a selective estrogen receptor modulator with anti-estrogenic activity in the mammary gland and is used as adjuvant therapy to prevent recurrence in hormone receptor–positive breast cancer13), it is known to have proliferative effects on the endometrium as an estrogen agonist and can induce endometrial polyps, endometrial hyperplasia, and endometrial carcinoma12,14). It is presumed that the onset of polypoid endometriosis after GnRH analogue administration is due to a rebound phenomenon upon withdrawal of GnRH agonist-induced hormone suppression8). In our case, it was speculated that polypoid endometriosis may have been triggered by treatment with a GnRH agonist (leuprorelin, 1.88 μg) administered for 4 months prior to the initial laparoscopic surgery to treat uterine fibroids.
The diagnosis of polypoid endometriosis is difficult to make based on imaging findings alone because of the variety of lesion shapes and onset sites, but there have been some reports that MRI is useful3,15,16). The solid component of polypoid endometriosis lesions has been shown to exhibit isosignal intensity, with some punctate high signal intensity on T1-weighted images (T1-WI) and high signal intensity on T2-weighted images (T2-WI), reflecting abundant endometrial glands and resembling endometrial polyps. However, these findings are not specific for polypoid endometriosis, and it is often difficult to diagnose polypoid endometriosis, including distinguishing it from malignancy, based on contrast effects and findings of diffusion restriction15). PET-CT may show increased FDG uptake in the area of polypoid endometriosis lesions, but this is not a specific finding and is not a diagnostic indicator of malignancy, as it may be related to increased uptake by inflammatory cells, as is sometimes seen in foci of endometriosis6,17).
In retrospect, the MRI findings in our case were relatively specific for polypoid endometriosis, with Tl-WI showing isosignal intensity with some high signal intensity, T2-WI showing high signal intensity, and PET-CT showing faint accumulation. However, before surgery we strongly suspected ovarian cancer with invasion and dissemination due to the rapid growth of the right adnexal tumor, the presence of a substantial growth (cecal tumor), and a large omental tumor that was suspected to represent metastasis. Therefore, we considered it difficult to perform primary debulking surgery in the second operation (first laparotomy), and instead performed exploratory laparotomy for preoperative chemotherapy and biopsied the omental tumor, a right ovarian tumor, and a tumor of the Douglas pouch. In fact, the uterus, rectum, sigmoid colon, right adnexal tumor, and ileocecal tumor were attached together by adhesions in the pelvic cavity, making it difficult to remove the tumors even if they were benign.
Although 4 months of treatment with a GnRH antagonist resulted in shrinkage of the right adnexal tumor, the ileocecal tumor remained unchanged. Furthermore, it was difficult to determine whether the ileocecal tumor was malignant because the endoscope could not pass through the sigmoid colon due to stenosis at the site of stent insertion. The third surgery (second laparotomy) was performed because ileal resection was deemed desirable given the risk of future stenosis or obstruction in the area. However, because the patient consistently refused to receive a colostomy under any circumstances, hysterectomy (with rectal and sigmoid colectomy) was not performed.
Colonoscopy after the second laparotomy showed persistence but no enlargement of the multiple polypoid tumors in the sigmoid colon, and bowel movements remained controllable with laxatives. It is unlikely that the patient’s endometriosis will worsen in the future because both ovaries were removed and blood estradiol levels have remained low (<10 ng/ml). As mentioned above, since there have been reports of postmenopausal polypoid endometriosis cases4) and of malignant transformation of postmenopausal ovarian endometrial cysts or ectopic endometriosis18), we believe that continued close follow-up is warranted in the present case.
Conclusion
Although a retrospective review of the MRI, PET-CT, and other imaging findings in this case were relatively typical for polypoid endometriosis, we strongly suspected advanced ovarian cancer before surgery and did not make the diagnosis of polypoid endometriosis. We regret that the lack of awareness of polypoid endometriosis was one reason why this diagnosis was not made preoperatively.
Conflict of interest
The authors have no conflicts of interest to declare.
Patient consent
We obtained informed consent from the patient for publication of this work.