

Endometrial cancer is the sixth most common malignant disease in the world and its incidence is increasing, particularly in developed countries1). Although the number of deaths has also been on the rise, the majority of endometrial cancers are diagnosed early and the prognosis is good1). However, 13% of cases show recurrence after treatment, among which 39% have tumor localization, such as in the vagina or pelvis2). Surgical treatment for pelvic locoregional recurrent tumors is an option for radical cure, but as many clinicians have pointed out, a high incidence of complications and negligible impact on prognosis can occur without complete resection3-5). The therapeutic efficacy of radiotherapy and chemotherapy for recurrent tumors has been limited6,7), raising expectations for novel therapeutic strategies. In this context, the efficacy of immune checkpoint inhibitors was confirmed and pembrolizumab was approved by the Food and Drug Administration (FDA) in 20178). Herein we describe a case of long-term control of otherwise treatment-refractory recurrent endometrial cancer in a patient who was administered pembrolizumab after cytoreductive surgery with pelvic exenteration. Written consent was obtained from the patient for permission to use the clinical information and images presented in this case report.
The content of research paper
Successful management of pelvic recurrence of MSI-High endometrial cancer by total pelvic exenteration followed by administration of pembrolizumab:A case report
Manabu Kojima, Shu Soeda, Chikako Okabe, Tetsu Sato, Norihito Kamo, Makiko Ueda, Yuta Endo, Shinji Nomura, Emi Tokuda, Shigenori Furukawa, Masao Kataoka, Shotaro Fujita, Shigehira Saji, Takafumi Watanabe, Keiya Fujimori
-
Manabu Kojima
Department of Obstetrics and Gynecology, Fukushima Medical University School of Medicine
-
Shu Soeda
Department of Obstetrics and Gynecology, Fukushima Medical University School of Medicine
-
Chikako Okabe
Department of Obstetrics and Gynecology, Fukushima Medical University School of Medicine
-
Tetsu Sato
Department of Obstetrics and Gynecology, Fukushima Medical University School of Medicine
-
Norihito Kamo
Department of Obstetrics and Gynecology, Fukushima Medical University School of Medicine
-
Makiko Ueda
Department of Obstetrics and Gynecology, Fukushima Medical University School of Medicine
-
Yuta Endo
Department of Obstetrics and Gynecology, Fukushima Medical University School of Medicine
-
Shinji Nomura
Department of Obstetrics and Gynecology, Fukushima Medical University School of Medicine
-
Emi Tokuda
Department of Medical Oncology, Fukushima Medical University School of Medicine
-
Shigenori Furukawa
Department of Obstetrics and Gynecology, Fukushima Medical University School of Medicine
-
Masao Kataoka
Department of Urology, Fukushima Medical University School of Medicine
-
Shotaro Fujita
Department of Gastrointestinal Tract Surgery, Fukushima Medical University School of Medicine
-
Shigehira Saji
Department of Medical Oncology, Fukushima Medical University School of Medicine
-
Takafumi Watanabe
Department of Obstetrics and Gynecology, Fukushima Medical University School of Medicine
-
Keiya Fujimori
Department of Obstetrics and Gynecology, Fukushima Medical University School of Medicine
Introduction
Case presentation (Table 1)
A 51-year-old Japanese woman with pelvic recurrence of endometrial cancer was referred to our hospital in June 2018. She underwent abdominal total hysterectomy, bilateral adnexectomy, and pelvic lymphadenectomy for endometrial cancer at another hospital in October 2016. The histopathological diagnosis was mixed adenocarcinoma arising from the endometrium (90% endometrial cancer grade 2 and 10% clear cell carcinoma), pT1aN0M0, stage IA, based on the International Federation of Gynecology and Obstetrics 2008 classification. The patient received six cycles of adjuvant chemotherapy with doxorubicin (50 mg/m2) and cisplatin (60 mg/m2) every three weeks. Computed tomography (CT) imaging after chemotherapy showed no evidence of disease and the patient was placed under surveillance. Unfortunately, a year after the last chemotherapy, the patient had recurrent tumor in the pelvis and surgical resection was performed, but the tumor could not be completely excised. The patient received three cycles of postoperative chemotherapy with paclitaxel (175 mg/m2) and carboplatin (area under curve 6) every three weeks, but the tumor grew again in the pelvis. CT images showed a 5 cm-sized recurrent tumor involving the bladder and rectum (Figure 1). The patient was referred to our hospital for treatment.
We performed external beam radiotherapy for the recurrent pelvic tumor, with only partial response. We then performed total pelvic exenteration in January 2019 for radical resection of the tumor along with the bladder, rectum, and vagina. Urinary diversion with ureterocutaneous fistula, intestinal end-to-end anastomosis, and colostomy were also performed. The bowel was edematous due to the adverse effects of radiotherapy and densely adherent to the pelvic wall. Most of the tumor was resected, but the adhesions precluded complete resection. In addition to the pelvic tumor, there were unresectable disseminated lesions in the mesentery of the small intestine. Total operative time was 15 hours, with total blood loss around 2000 mL. The resected tumor had invaded the bladder and rectum (Figure 2). Microscopically, the tumor cells had clear cytoplasm and a hobnail-like appearance (Figure 3), and immunostaining was positive for cytokeratin AE1/3 and hepatocyte nuclear factor (HNF)-1β, weakly positive for p53, and negative for estrogen receptor (ER), supporting the diagnosis of clear cell carcinoma. The tumor showed high microsatellite instability (MSI-High). The patient did not have a family history of cancer. Postoperative complications such as surgical site infection occurred, but were not serious, and the patient was discharged 66 days after surgery. A CT scan performed two months after surgery showed that the recurrent tumor had been almost completely resected, but a portion of the tumor persisted in the pelvic wall. Given that the tumor was MSI-High, medication with pembrolizumab (200 mg every 21 days) was started three months after surgery. A reduction in the remaining tumor size in the pelvic wall was observed by CT scan performed three months after the initiation of pembrolizumab (Figure 4). At the time of this report, treatment with pembrolizumab has been ongoing, and the residual tumor mass has remained reduced for 32 months since the start of treatment (Figure 5). The patient’s liver function, blood glucose, and thyroid and parathyroid functions have been monitored since before the start of pembrolizumab treatment; pathological changes that require therapeutic intervention have not been observed thus far. No serious adverse events have emerged that would warrant discontinuation of treatment.
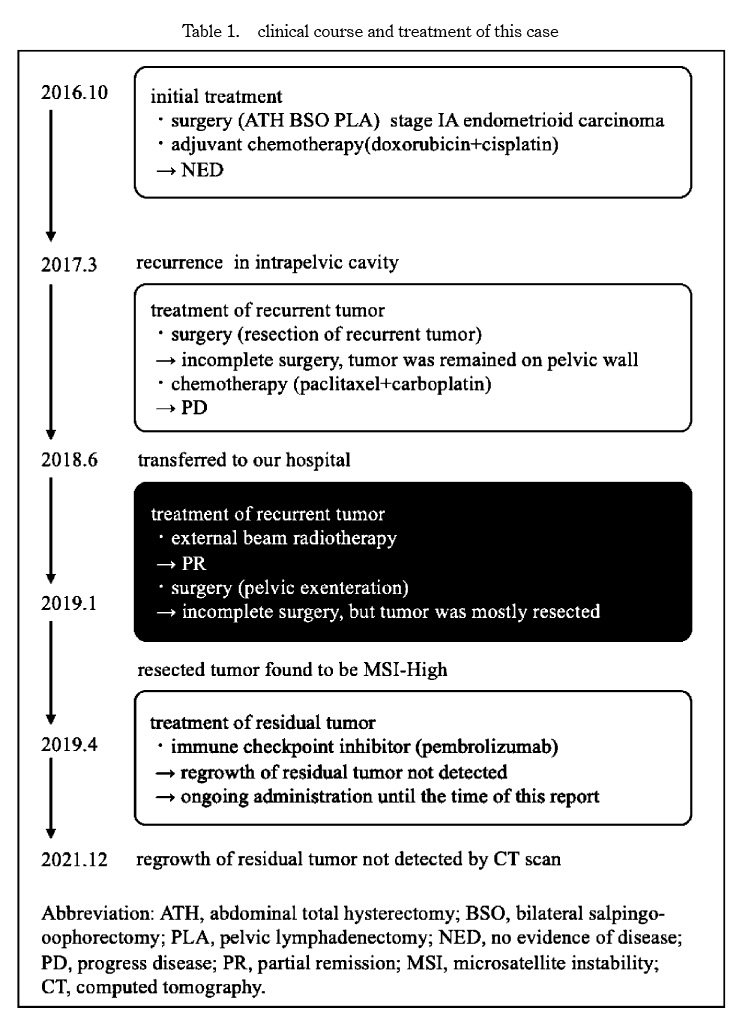
Table 1. clinical course and treatment of this case
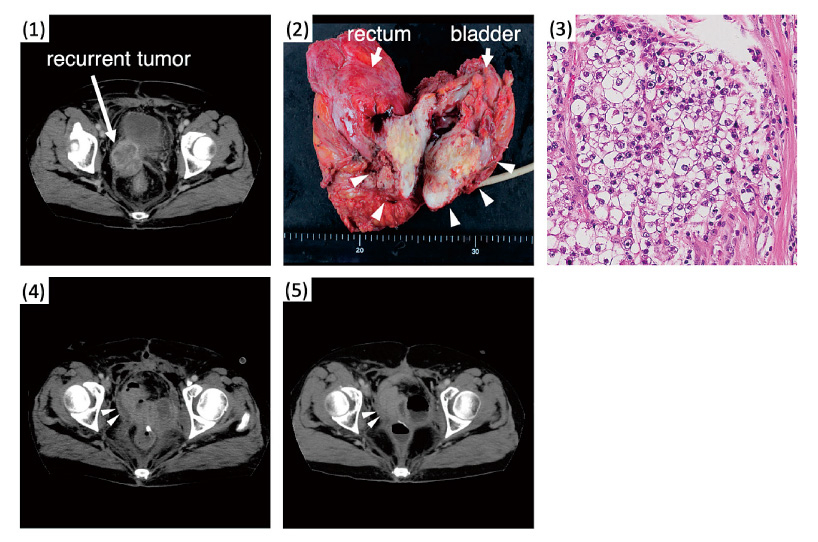
Fig. 1. CT images showed a 5 cm recurrent tumor involving the bladder and rectum.
Fig. 2. Resected tumor. Invasion into the bladder and rectum was observed.
(Arrowheads indicate the recurrent pelvic tumor.)
Fig. 3. Hematoxylin-eosin staining (×200) revealed that the tumor cells had clear cytoplasm and a hobnail-like appearance.
Fig. 4. Post-operative CT images showed that the recurrent tumor mass in the pelvis had been surgically reduced.
(Arrowheads indicate the slight residual pelvic tumor.)
Fig. 5. At 32 months after the start of pembrolizumab treatment, the tumor remained reduced in size on CT.
(Arrowheads indicate the slight residual pelvic tumor.)
Discussion
In this case report, we described a patient with endometrial cancer who had long-term survival after pelvic exenteration for treatment-refractory recurrent pelvic tumor. The treatment options for recurrent endometrial cancer are surgery, radiotherapy, kkchemotherapy, and hormone therapy. Systemic or multiple recurrence is treated with chemotherapy, but the response of recurrent endometrial cancer to chemotherapy is unsatisfactory, with response rates ranging from 21% to 36% for any drug7). Furthermore, as many clinicians have experienced, even if the tumor does respond to chemotherapy, it eventually becomes uncontrollable. Hormone therapy with progestin is known to have a high response rate, but has the disadvantage of being limited to estrogen and progesterone receptor-positive tumors, such as endometrioid carcinoma grade 19). Recurrent tumors that have become resistant to chemotherapy and hormone therapy have a severe prognosis if they cannot be treated radically with surgery or radiotherapy10). Locoregional recurrence in the pelvis is treated with surgery if resection is possible, whereas radiotherapy is also a treatment option if there is no history of radiotherapy to the pelvis11). However, it should be noted that the complete remission rate with radiotherapy is only 40% for pelvic recurrence compared to 89% for vaginal recurrence12). Surgery may be considered for tumors that have become refractory to radiotherapy, but many previous studies have concluded that incomplete resection is not conducive to the prognosis of patients, and surgical techniques such as total pelvic exenteration, which is highly invasive and has a high rate of complications3-5), need to be selected appropriately with due regard to imaging and performance status. In the present case, it is remarkable that the residual tumor has remained stable for more than two years without regrowth.
This patient has had a favorable course that we attribute to response of the residual tumor to pembrolizumab. Pembrolizumab is a programmed cell death protein-1 signal pathway inhibitor that was administered in the KEYNOTE-158 study to patients with unresectable locally advanced or metastatic solid tumors with MSI-High or deficient mismatch repair (dMMR) that had been treated with standard chemotherapy13). The patients who received pembrolizumab had an objective response rate (ORR) of 34.3% and a progression-free survival (PFS) of 4.1 months. Patients with endometrial cancer showed a favorable outcome with an ORR of 57.1% and a median PFS of 25.7 months. Pembrolizumab was approved by the FDA in 2017 and has been administered in Japan since 2018 for solid tumors that are treatment-refractory and MSI-High. Chan et al. reported two cases of multi-metastatic endometrial cancer that had become refractory to chemotherapy14). In these two cases, pembrolizumab reduced the tumor size and the cancer was controlled for more than two years.
Furthermore, a unique aspect of treatment in the present case was the use of pelvic exenteration to reduce the recurrent tumor mass prior to the administration of pembrolizumab. Although complete resection of the residual tumor was not achieved, most of the tumor was resected. Regarding radiotherapy and chemotherapy for advanced and recurrent tumors, it is known that the smaller their diameters are, the better the treatment outcome is12,15).
On the other hand, we have not seen such reports in the context of treatment with immune checkpoint inhibitors such as pembrolizumab. Therefore, it is not known whether the cytoreductive surgery we performed on this patient contributed to the long-term response to pembrolizumab.
Conclusion
This patient with MSI-High endometrial carcinoma refractory to chemotherapy and radiotherapy was treated with pelvic exenteration followed by pembrolizumab. Follow-up thus far shows a successful outcome. For patients with MSI-High endometrial cancer, pembrolizumab therapy is potentially an effective treatment modality that can contribute to long-term tumor control. To answer whether or to what extent cytoreductive surgery contributes to the efficacy of pembrolizumab will require further case reports and careful analysis.