Low back pain (LBP) is highly prevalent in developed countries, where two thirds of adults have been affected by back pain1). LBP is associated with high health care costs and the loss of productivity, and is considered to have an economic impact2). In addition, it is widely known that LBP affects depression3) and quality of life (QOL). Therefore, it is important to investigate the causes of LBP.
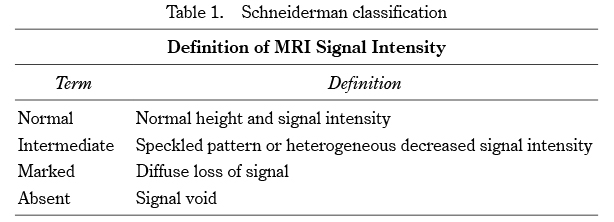
Magnetic resonance imaging (MRI) is a non-invasive and accurate method for morphological evaluation of the lumbar spine4). It is appropriate for assessing the association between the morphological findings on imaging and LBP5), and is commonly performed in current LBP practice. Disc degeneration (DD) can be visualized as an abnormal finding on MRI. Histologically, DD is a state of reduced water content and motility due to reduced proteoglycan content and fibrosis in the nucleus pulposus4,6). Such degeneration is apparent as decreased T2 signal intensity in the disc and narrowing of the intervertebral height on MRI. Intervertebral DD is known to involve both age-related changes and tissue damage brought on by combined stresses, including those from mechanical, nutritional, and chemical factors7,8). However, the relationship between DD and LBP remains controversial. Numerous previous studies have suggested that DD on MRI is related to the presence of LBP5,9-13). DD is commonly observed as age-related change in asymptomatic subjects14-16), but abnormal DD that is not appropriate for age may be symptomatic. Previous cross-sectional studies in the general population have suggested that DD is an age-related phenomenon17-20), although a small percentage of young people have multiple DD whereas some older people do not have DD19). It has been suggested that some DD is related to factors other than age, such as genetics, nutrition, and trauma5,21,22). Several case-control studies in young subjects have suggested a relationship between DD and LBP5,23,24). Advanced DD in young people is thought to indicate pathological degeneration that may be associated with symptoms. Several problems can be identified in previous studies of the relationship between DD seen on imaging and LBP. The first is the evaluation of symptomatic and asymptomatic DD as a single category. Age-related DD in the elderly and more rapidly progressive DD in the young may have different pathologies and should be evaluated separately. The lack of assessment of the characteristics of LBP is another problem. Complaints of LBP vary widely and are reported to be associated with psychosocial factors25). LBP due to psychosocial factors may not be based on abnormal findings on imaging. In addition to the presence or absence of LBP, it is also important to assess LBP-specific QOL and health-related QOL. The purpose of this study was to investigate the association between LBP and DD in community residents using a detailed assessment of LBP, and to investigate whether there is an association between age-appropriate and age-inappropriate DD and LBP.