

The Pfizer-BioNTech BNT162b2 vaccine effectively protects individuals from SARS-CoV-2 infection1,2). However, data are still being accumulated to determine the timing of the peak and duration of antibody production following immunization with this specific vaccine. This study investigated the immune response and other outcomes related to BNT162b2 vaccination among hospital staff in Fukushima, Japan.
This observational study was conducted in a small group of Japanese hospital workers after approval from the Ethics Committees of Hirata Central Hospital (number 2021-0611-1) and Fukushima Medical University (number 2021-116). Blood samples were collected from participants before their first vaccination to assess prior exposure to SARS-CoV-2. Specifically, immunoglobulin M antibody against SARS-CoV-2 N-protein was measured to confirm that no participants had been infected with SARS-CoV-2. Subsequent sampling was performed during the participants’ working days (5 days “on” + 2 days “off”) for six weeks after their first vaccination. Demographic information was obtained from medical records of the participants and further information on medical history and adverse reactions following vaccination were obtained through a questionnaire. First doses of BNT162b2 were given April 19-23, 2021 and second doses were given May 10-14, 2021 (21 days apart and according to the manufacturer’s instructions).
Post-vaccination titers of immunoglobulin G (IgG) antibody against SARS-CoV-2 spike (S1) protein were measured via a chemiluminescent immunoassay using a high-throughput assay apparatus (iFlash 3000, YHLO Biotech, Shenzhen, China) at the University of Tokyo, June 21-23, 2021. Pre-vaccination immunoglobulin M (IgM) antibody against SARS-CoV-2 nucleocapsid (N) protein was measured for evidence of past SARS-CoV-2 infection, using the same method as for IgG antibody titers against S1 protein. The cut-off value of each test was 10 arbitrary units per milliliter, with testing conducted according to official guidelines.
The mean and standard deviation of IgG antibody titers were evaluated as a whole, by age group (12 staff divided into the six eldest and six youngest), and by sex.
The median age of the six male and six female participants was 45 years (range 22-61 years). The 12 individuals comprised seven (58%) medical staff and five (42%) non-medical staff. Five (42%) had pre-existing conditions (i.e., hypertension, dyslipidemia, thyroid disease, and ovarian disease). Six individuals had at least one systemic adverse reaction (e.g., joint pain, fatigue, headache) after their first vaccination dose. Nine individuals had at least one systemic adverse reaction, including a fever over 37.5°C, joint pain, fatigue, and/or headache after their second dose. Of these, five individuals had a fever over 37.5°C. All participants tested negative for IgM antibody against SARS-CoV-2 N protein prior to vaccination; thus, we concluded that no one had a past SARS-CoV-2 infection history.
The mean IgG antibody titer was under 1.0 until day 8, becoming higher than the cut-off value at day 11 (Figure 1). It began significantly increasing three days after the second vaccination. Our data showed antibody titers peaking 6-13 days after the second vaccination (days 27-34 from the first), with a steady decrease thereafter (Figure 1).
The group of six elder individuals (median age 53 years) had lower antibody titers than the group of six younger individuals (median age 35 years), and the male group had lower antibody titers than the female group (Figures 2a and 2b). The mean peak antibody titers were 2,414 for the elder group and 3,101 for the younger group (p=0.24 with t-test, Figure 2a), 2,386 for males and 3,469 for females (p=0.016 with t-test, Figures 2b), and 2,485 for those afebrile and 2,764 for those febrile after vaccination (p=0.26 with t-test, data not shown). A statistically significant difference in antibody titers emerged only between males and females.
A marked increase in IgG antibody against SARS-CoV-2 S1 protein was observed after the second dose of the BNT162b2 vaccine. IgG antibody titers appeared to peak 6- 13 days after the second vaccination before gradually diminishing. The mean titer of IgG antibody against the S1 protein was 3,016 on day 34, decreasing to 2,136 by day 42. The regression line between days 28 and 42 projects a mean titer of zero by day 103.
IgG antibody titers appeared to peak 6- 13 days after the second vaccination, with antibody titers higher among females. Differences in IgG antibody against S1 protein titers observed between groups, according to age, gender, and post-vaccination adverse events, concurs with previous studies3,4). Previous studies have shown that people with compromised immune systems, such as organ transplant recipients, may require a third vaccine dose to achieve appropriate antibody titers5). Further research is needed to fully evaluate the relationship between antibody levels and infection with SARS-CoV-2 viral strains.
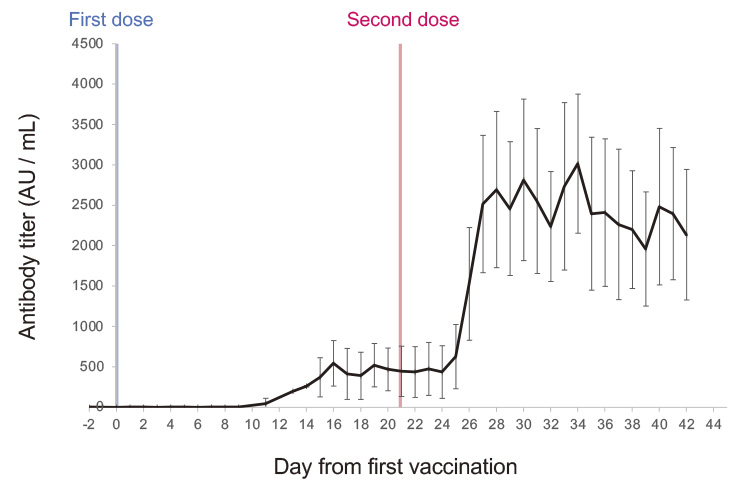
Fig. 1. Mean and standard deviation of IgG-antibodies against S1-protein titer for all.
Initial blood sampling was performed before the first vaccination to monitor the sequential titer of IgG antibody against SARS-CoV-2 S1-protein. Subsequent blood sampling was performed approximately 20 times for each staff participant until 42 days after the first vaccination.
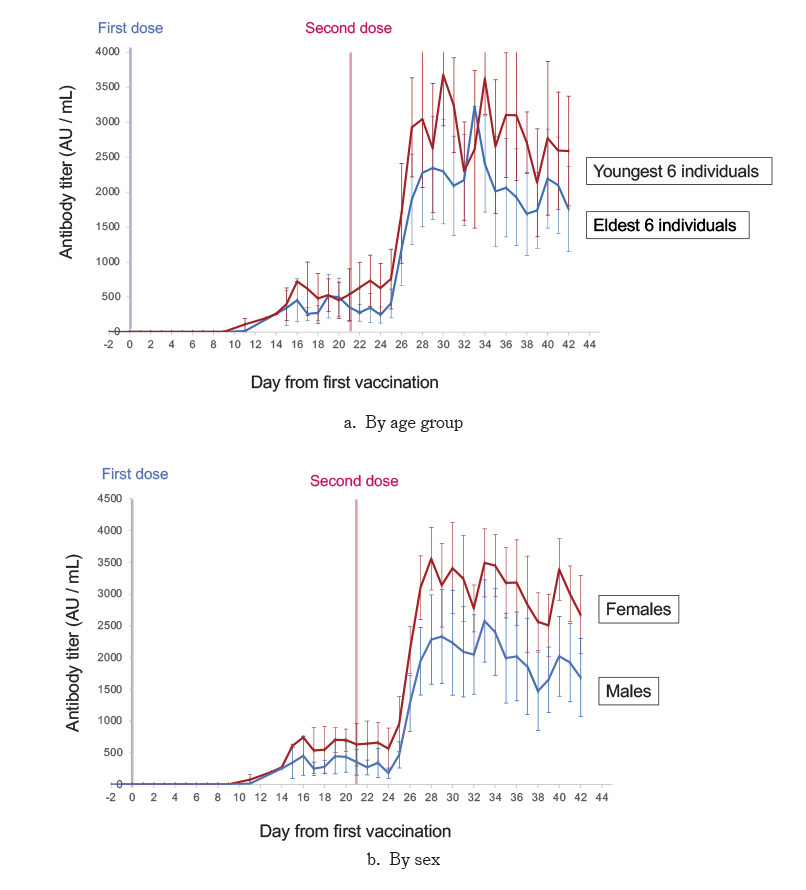
Fig. 2. Mean and standard deviation of IgG-antibodies against S1-protein titer by age (2a), and by sex (2b).
Twelve staff members were divided into groups consisting of the six eldest and six youngest, six males and six females.