

The Bentall procedure1). is the gold-standard treatment for aortic root pathologies and is now used worldwide. This procedure is a reliable technique for many cardiac surgeons and its reported clinical results are acceptable2-10). We applied the modified Bentall procedure in which coronary reconstruction was performed by the Carrel button technique as the first choice for patients with aortic root pathologies. We also applied the flanged technique to construct a composite graft11). In this study, we evaluated the early and long-term results of modified Bentall procedures with the flanged technique and discussed indications for bio- and mechanical Bentall procedures.
The content of research paper
Long-term results of modified bentall procedures: 18-year experience of the flanged technique
Takashi Igarashi, Hirono Satokawa, Yoichi Sato, Shinya Takase, Hiroki Wakamatsu, Yuki Seto, Hiroyuki Kurosawa, Masumi Iwai-Takano, Tsuyoshi Fujimiya, Hiroharu Shinjo, Keiichi Ishida, Hitoshi Yokoyama
Author information
-
Takashi Igarashi
Department of Cardiovascular Surgery, Fukushima Medical University
-
Hirono Satokawa
Department of Cardiovascular Surgery, Fukushima Medical University
-
Yoichi Sato
Department of Cardiovascular Surgery, Yonezawa City Hospital
-
Shinya Takase
Department of Cardiovascular Surgery, Fukushima Medical University
-
Hiroki Wakamatsu
Department of Cardiovascular Surgery, Fukushima Medical University
-
Yuki Seto
Department of Cardiovascular Surgery, Fukushima Medical University
-
Hiroyuki Kurosawa
Department of Cardiovascular Surgery, Fukushima Medical University
-
Masumi Iwai-Takano
Department of Cardiovascular Surgery, Fukushima Medical University
-
Tsuyoshi Fujimiya
Department of Cardiovascular Surgery, Fukushima Medical University
-
Hiroharu Shinjo
Department of Cardiovascular Surgery, Fukushima Medical University
-
Keiichi Ishida
Department of Cardiovascular Surgery, Fukushima Medical University
-
Hitoshi Yokoyama
Department of Cardiovascular Surgery, Fukushima Medical University
Introduction
Patients and methods
This was a retrospective single-center study. Informed consent was obtained from all patients at initial admission. Our institutional review board approved this study (approval number: 2019-238).
Patients
We reviewed the medical records of 63 patients who had undergone root replacement by the modified Bentall procedure at our institute between January 2001 and December 2018 (mean age 57 ± 16 years, range 16-80, male 43 cases). The mean follow-up was 75 ± 56 months (range 0-216). Through April 1, 2020, we could follow up on 61 cases (97%).
Surgical Procedures
Under general anesthesia and mechanical ventilation, the chest was opened via the median full-sternotomy approach. Extracorporeal circulation was established by perfusion from the ascending aorta and drainage from the superior and inferior vena cava. A left ventricular vent was inserted from the right superior pulmonary vein. During cross-clamping of the ascending aorta, antegrade and retrograde blood cardioplegia was administered every 20 minutes to maintain cardiac arrest. We used a composite graft, which was prepared in the operating room using an artificial aortic valve and a Dacron graft, in most cases. A bioprosthesis was selected if a patient was older than 65 years old. In younger patients, a mechanical valve was used. As a result, 26 patients underwent the bio-Bentall procedure. The choice of valve model was up to the surgeon. The valve size was selected according to the patient’s body surface area, securing enough effective orifice area. A graft 3-5 mm larger than the valve was used. Until the introduction of the Valsalva graft (ValsalvaTM Ante-Flo, TERUMO, Tokyo, Japan) in April 2011, we used a straight Dacron graft. A composite graft was then constructed by the flanged technique as reported by Yakut11). Everting pledgeted 2-0 polyester sutures were placed on the aortic annulus and passed through the Valsalva graft collar below the sewing cuff of the valve prosthesis (Figure 1a, b). To secure hemostasis of the aortic annulus, an additional running suture with 4-0 polypropylene was performed at the proximal anastomosis of the graft (Figure 1c). The coronary ostiums were trimmed with a 7-mm long cuff of the aortic wall and were anastomosed with a 5-0 polypropylene running suture by the Carrel button technique. In cases with bioprosthesis, anticoagulation therapy with warfarin was maintained for 3 months as the postoperative antithrombotic therapy.
Antiplatelet therapy was then continued with aspirin.
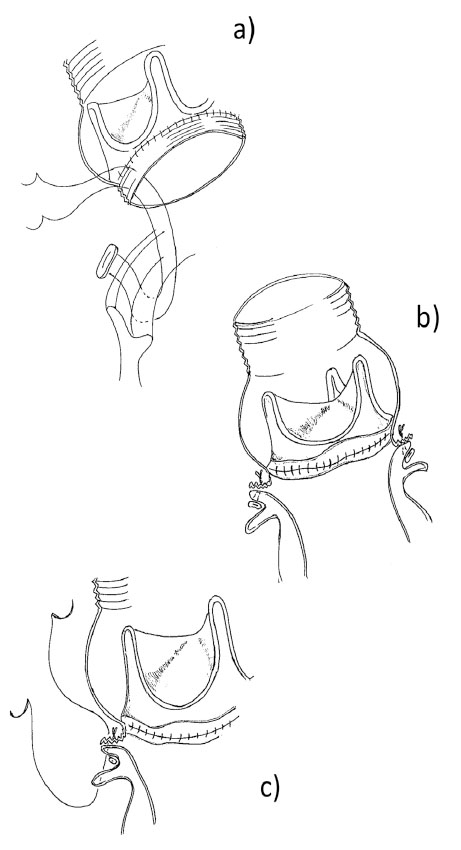
Fig. 1. Flanged technique using composite graft (bioprosthesis and Valsalva graft).
1a and 1b) Everting pledgeted 2-0 polyester sutures were placed on the aortic annulus and passed through the Valsalva graft collar below the sewing cuff of the valve prosthesis.
1c) To secure hemostasis of the aortic annulus, an additional running suture with 4-0 polypropylene was performed at the proximal anastomosis of the graft.
Follow-up
After discharge, the patients received regular medical follow-up at our hospital or outpatient clinic. The patients’ condition was checked by medical record, direct telephone interview, and questionnaire research.
Definitions of Major Adverse Valve-Related Events
Major adverse valve-related events include the following: (1) valve-related mortality; (2) all valve-related morbidity (structural valve deterioration, nonstructural dysfunction, valve thrombosis, embolism, bleeding events, operated valve endocarditis, and reintervention); and (3) need for a new permanent pacemaker or defibrillator within 14 days after the valve intervention12).
Echocardiographic Evaluation
Ventricular and valvular functions were evaluated with transthoracic echocardiography using standard views according to current guidelines13). Aortic regurgitation and stenosis were graded as mild, moderate, moderate-severe, and severe. Moderate aortic stenosis was defined as a mean systolic aortic valve pressure gradient of ≥ 20 mmHg14).
Statistical Analysis
Statistical analysis was performed using the Statistical Package for Social Sciences, ver. 25 (SPSS Inc., Chicago, Illinois, USA). Preoperative characteristics, operative data and postoperative early results were analyzed. Data were expressed as means ± standard deviation with range for continuous variables. Categorical variables were expressed as numbers and percentages. In the univariable analyses, continuous and categorical variables were compared using the Student’s t-test, χ2, or Fisher’s exact test as appropriate (Fisher’s exact test was used only when one of the four cells of a 2×2 table had less than five observations). Survival curves were estimated using the Kaplan-Meier method. All tests were two-sided, with statistical significance set at 0.05.
Results
Perioperative Data and Early Results
Preoperative patient characteristics are summarized in Table 1. Twenty-eight patients (44%) with annulo-aortic ectasia, 19 (30%) with root aneurysm, 12 (19%) with aortic dissection, 3 (5%) with bicuspid aortic valve, 37 (59%) with more than moderate aortic regurgitation, 5 (8%) with infective endocarditis, 3 (5%) with root abscess, and 11 (18%) with Marfan syndrome were included in our study. Table 2 shows the operative data and early results. As a concomitant procedure, coronary artery bypass grafting (12 cases, 19%), aortic arch repair (6 cases, 10%) and other valve procedure (8 cases, 13%) were performed. The Valsalva graft was used in 19 cases (30%). The aorta cross-clamping time was 197 ± 62 minutes. The extracorporeal circulation time was 256 ± 97 minutes. Hospital mortality was 7.9%. Mortality of elective surgery was 4.8%. The causes of in-hospital death were as follows: one systemic inflammatory response syndrome, one pneumonia, one multiple organ failure due to low output syndrome, one sepsis and one intestinal ischemia due to aortic dissection.
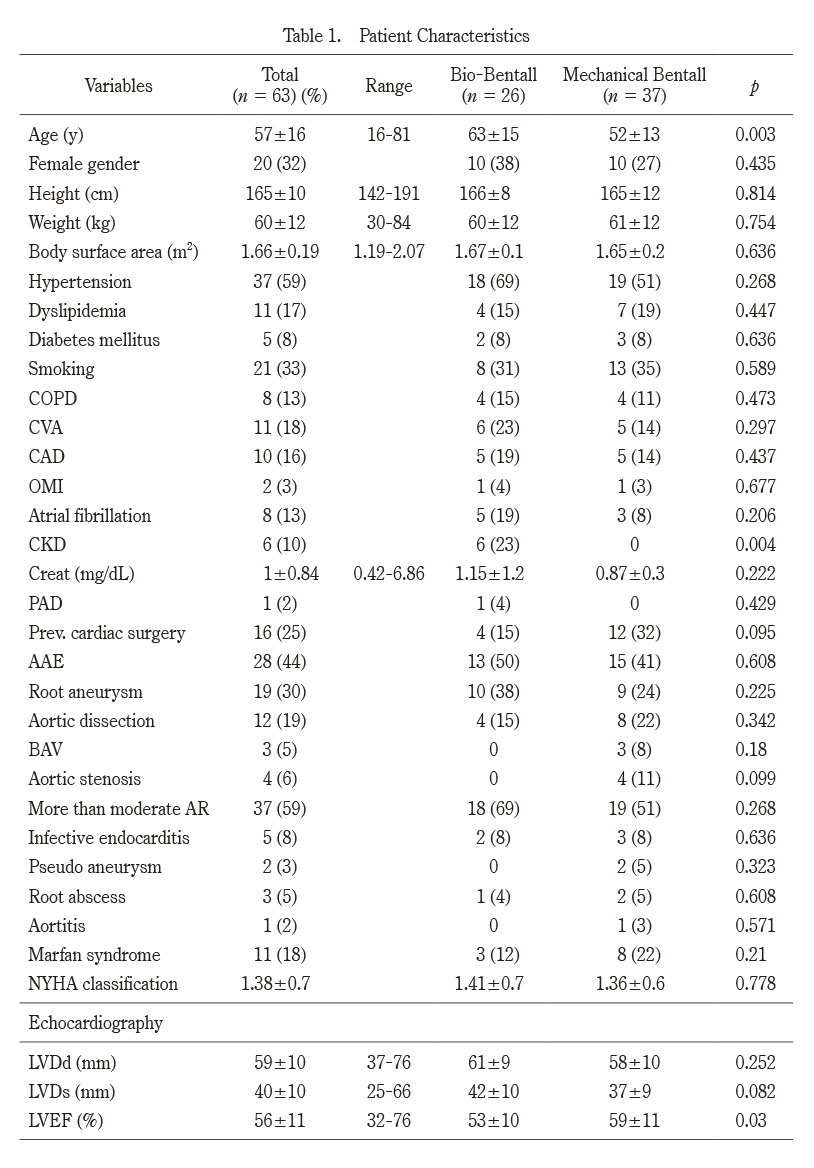
Table 1. Patient Characteristics
AAE, annuloaortic ectasia;AR, aortic regurgitation;BAV, bicuspid aortic valve;CAD, coronary artery disease;CKD, chronic kidney disease;COPD, chronic obstructive pulmonary disease;CVA, cerebrovascular accident;LVDd, diastolic left ventricular diameter;LVDs, systolic left ventricular diameter;LVEF, left ventricular ejection fraction;OMI, old myocardial infarction;PAD, peripheral artery disease.
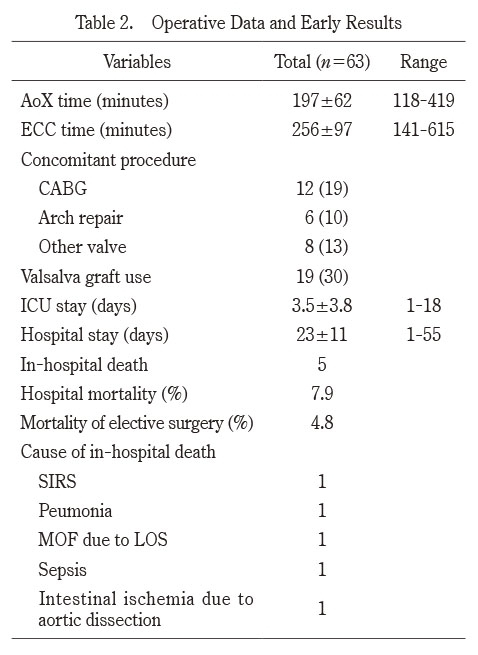
Table 2. Operative Data and Early Results
AoX, aorta cross-clamp; CABG, coronary artery bypass grafting; ECC, extracorporeal circulation; ICU, intensive care unit;LOS, low output syndrome; MOF, multiple organ failure;SIRS, systemic inflammatory response syndrome.
Valve Size of Bioprosthesis
The type and number of bioprostheses and mechanical valves are summarized in Table 3. Carpentier-Edwards Perimount bioprosthesis 25 mm in size was most frequently used (10 cases, 38%) in patients who underwent the bio-Bentall procedure.
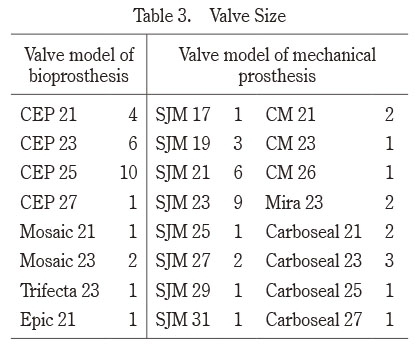
Table 3. Valve Size
CEP, Carpentier-Edwards Perimount;SJM, St. Jude Medical;CM, Carbomedics
Long-Term Results in Late Follow-up
Table 4 shows the long-term results in late follow-up. Eight deaths were observed in the late follow-up. In the bio-Bentall group, only two patients died due to cancer, and there were no deaths caused by cardiac or cerebrovascular events. However, in the mechanical Bentall group, six deaths, including one sudden death, one due to hemoptysis, one by congestive heart failure, and two during reoperations due to prosthetic valve endocarditis, were observed. In the bio-Bentall group, there were no major adverse cardiac or cerebrovascular events. In the mechanical Bentall group, two cerebral hemorrhages and one cerebral embolism were observed. Figure 2a shows the results of the Kaplan-Meier analysis regarding freedom from all-cause death. In the bio-Bentall group, the rate of freedom from all-cause death at 5 years was 94.1%, and the rates at 5 and 10 years in the mechanical Bentall group were 93.1% and 79.3%, respectively.
Figure 2b indicates the results of the Kaplan-Meier analysis regarding freedom from major adverse valve-related events (MAVREs). In the bio-Bentall group, the rate of freedom from cardiac events was 100% at 5 years, and the rates at 5 and 10 years in the mechanical Bentall group were 93.8% and 76.8%, respectively (one sudden death, one congestive heart failure, two reoperations due to prosthetic valve endocarditis, two cerebral hemorrhages, and one cerebral embolism).
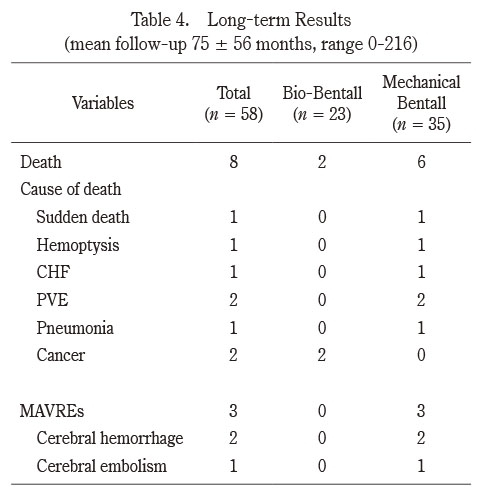
Table 4. Long-term Results (mean follow-up 75 ± 56 months, range 0-216)
CHF, congestive heart failure;MAVREs, major adverse valve-related events;PVE, prosthetic valve endocarditis.
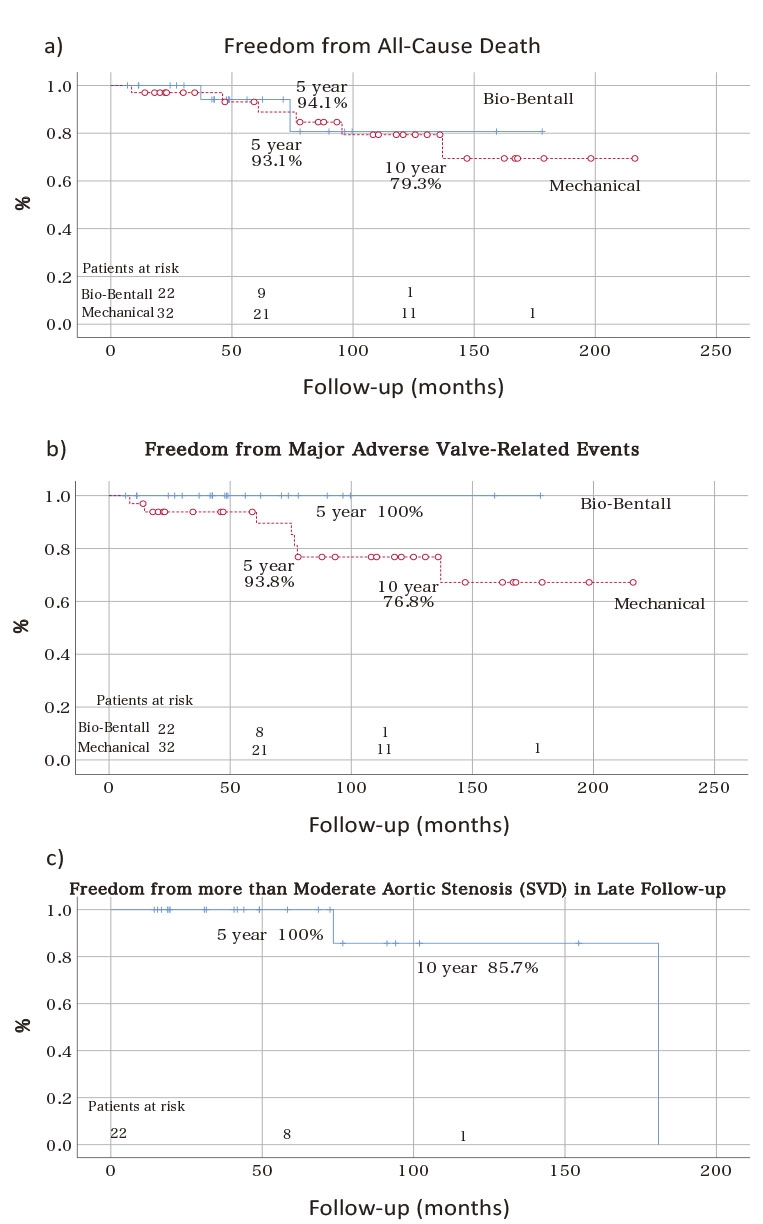
Fig. 2. Kaplan-Meier analysis of freedom from all-cause death, MAVRE, and SVD.
a) In the bio-Bentall group, the rate of freedom from all-cause death at 5 years was 94.1%, and the rates at 5 and 10 years in the mechanical Bentall group were 93.1% and 79.3%, respectively.
b) In the bio-Bentall group, the rate of freedom from cardiac events was 100% at 5 years, and the rates at 5 and 10 years in the mechanical Bentall group were 93.8% and 76.8%.
c) The rates of freedom from more than moderate aortic stenosis at 5 and 10 years in bio-Bentall group were 100% and 85.7%, respectively.
Valve Function of Bio-prosthesis in Late Follow-up
Echocardiographic follow-up was performed in 22 cases (96%) in the bio-Bentall group. Figure 2c shows the results of the Kaplan-Meier analysis regarding freedom from more than moderate aortic stenosis due to structural valve deterioration in the bio-Bentall group (n = 22). The rates of freedom from more than moderate aortic stenosis at 5 and 10 years were 100% and 85.7%, respectively. Figure 3 shows the results of the Kaplan-Meier analysis regarding freedom from severe aortic stenosis due to structural valve deterioration in the bio-Bentall group (n = 22). The rate of freedom from severe aortic stenosis due to SVD was 100% at both 5 years and 10 years.
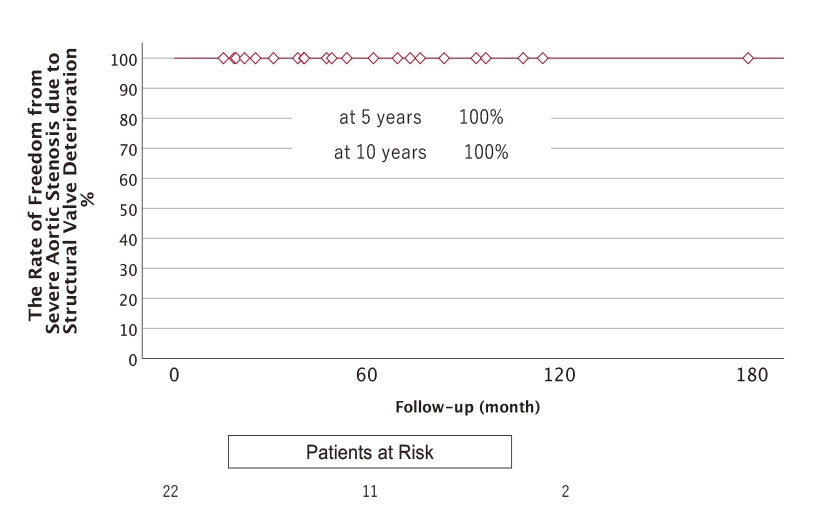
Fig. 3. The results of the Kaplan-Meier analysis regarding freedom from severe aortic stenosis due to structural valve deterioration in the bio-Bentall group. The rate of freedom from severe aortic stenosis due to SVD was 100% at both 5 years and 10 years.
Discussion
The Bentall procedure is standard therapy for aortic root pathologies. We have consistently performed the modified Bentall procedure for patients of aortic root replacement since 2001. The current study shows excellent long-term outcomes in late follow-up, especially among patients of the bio-Bentall procedure. During the follow-up, no MAVREs were observed in the patients who received the bio-Bentall procedure. Castrovinci et al. reported a systematic review of aortic root replacement with biological valved conduits3). They showed that the rates of freedom from all-cause death at 5 and 10 years were 76% and 58%, respectively, and the rate of freedom from reoperation at 5 years was 90%. In the current study, the rate of freedom from severe aortic stenosis due to structural valve deterioration was 100% at 10 years, an excellent result. Bourguignon et al. showed very long-term outcomes of the Carpentier-Edwards Perimount Valve in aortic position15). In that study, 2,559 patients underwent aortic valve replacement with Carpentier-Edwards Perimount Valve. The valve size was 19 mm in 384 patients (13.9%), 21 mm in 888 patients (32.2%) and 23 mm in 924 patients (33.5%). The rate of severe SVD (severe aortic stenosis or regurgitation) was 94.2% at 10 years and 78.6% at 15 years.
During the observation period, no reoperation was required among the patients who underwent the bio-Bentall procedure. The longer durability after the bio-Bentall procedure resulted in favorable long-term outcomes. These results may be due to the larger bioprosthesis used as the composite graft. In the cases using a larger bioprosthesis, it takes longer for clinically significant and/or symptomatic structural valve deterioration to occur. Issa et al. reported that small bioprosthesis size independently predicted structural valve deterioration16).
Johnston et al. reported a long-term series of Carpentier-Edwards Perimount aortic valves in aortic valve replacement17). Among their 12,569 patients, a 23-mm valve was most frequently used (n = 4,145, 33%), followed by a 21-mm valve (n = 3,385, 27%). Minakata et al. reported the long-term outcome of Carpentier-Edwards pericardial valves in the aortic position among Japanese patients18). In a total 591 patients who underwent aortic valve replacement, the 21-mm valve was most frequently used (n = 207, 38.3%), followed by the 23-mm valve (n = 154, 28.5%). In our study, a 25-mm Carpentier-Edwards bioprosthesis was more frequently used (10 cases, 38%), followed by the 23-mm valve (6 cases, 23%). The mean body surface area of our patients was 1.66 ± 0.19 m2)., which is around average for Japanese patients. Regarding the required effective orifice area, we could use relatively larger bioprostheses than in the isolated aortic valve replacement. The flanged technique was reported by Yakut et al.11). in 2001 as a new modification of the modified Bentall procedure. They described that this technique enables the aortic annulus to maintain its flexibility and elasticity, and facilitates the annular dilatation technique if needed. We began using the flanged technique to secure hemostasis at the proximal anastomosis. In addition, this technique contributes to enabling the use of a larger prosthesis than required. Tabata et al. also reported that their case series had undertaken a similar technique using a bioprosthesis and a Valsalva graft19). They described that this technique allows the surgeon to place a valve larger than the annulus, which especially helps patients with a small aortic annulus.
Chirichilli et al. reported their experience with the Bentall procedure using the Perimount bioprosthesis and the Valsalva graft20). In a total of 309 cases, a 25-mm valve was most frequently used (149 cases, 48%), followed by a 23-mm valve (101 cases, 33%). These results were similar to those of our study. The use of large-sized bioprostheses may have contributed to the good long-term outcomes.
During our echocardiographic follow-up, the severity of aortic stenosis was of very low grade in all cases except two. One of the patients (a 21-year-old woman, operated on for annulo-aortic ectasia using a Carpentier-Edwards perimount 25 mm and a straight Dacron graft) had moderate aortic stenosis 15 years after the initial operation.
In addition, the Valsalva graft may play a role in improving valve durability and decreasing valve-related complications. Chirichilli et al. found that the Valsalva graft with the presence of pseudosinuses appears to play a beneficial role in regulating aortic root blood flow and may potentially decrease the risk of coronary button complication. Furthermore, the presence of vortices tends to wash the transitional area between the prosthetic valve and the Dacron conduit, potentially decreasing the incidence of thromboembolism20). In our study, the Valsalva conduit was used in 19 patients (73%). We expect further improvement in long-term outcomes by means of the Valsalva graft. From the results of this study, at present, the bio-Bentall procedure is the first choice in our strategy for the patients over age 65 with aortic root pathologies.
After the mechanical Bentall procedure, thromboembolic complications and bleeding events can occur. Among our patients, there were two cases of cerebral hemorrhage and one of cerebral embolism. Although the mechanical valve was selected due to its long-term durability and for avoidance of reoperation, maintaining a quality of life is also important, especially in young patients who have long life-expectancy. Bouhout et al. showed that the survival of patients after mechanical AVR was inferior to that of the general population who were age- and sex-matched21). They concluded that AVR with a mechanical valve is the standard therapy for young patients; however, the outcomes were suboptimal. Our study suggests that life-long anticoagulation therapy in young patients should be avoided if possible. In this regard, valve-sparing aortic root repair (VSARR)22). and the Ross procedure23,24). have great advantages.
There are several limitations in our study. First, this study was a retrospective single-center study, and the sample size and the number of events were very small. Second, we could not have a comparison with propensity matching to clarify the difference between the bio-Bentall group and the mechanical Bentall group in terms of early and late outcomes. Third, we used several types of bio- and mechanical prostheses and were not able to identify differences among any prosthetic varieties. Finally, we could not make a comparison between the small and large bioprostheses in terms of their long-term durability.
Compliance with ethical standards
All authors declare that they have no conflicts of interest pertaining to this investigation.