Characteristics of the donors
Table 1 summarizes the characteristics of the ten donors. The median patient age was 47 years (18-59 years). Six donors were > 45 years old. The median BMI was 22.8 kg/cm2 (17.3-28.4), and the median HbA1c level was 5.6% (5.1-6.1). Brain death was caused by head trauma in four patients, anoxic brain injury in four, and cerebrovascular accident (CVA) in two. Three donors had histories of cardiopulmonary arrest (CPA) that required resuscitation. Half of the donors had unstable hemodynamics, which necessitated the administration of high doses or multiple vasopressors. All but one case involved marginal donors as defined by Kapur’s criteria.16)
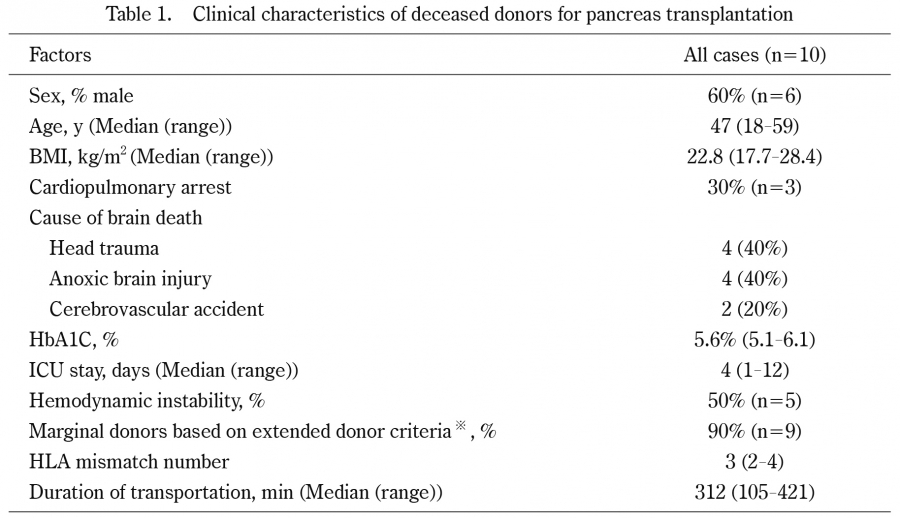
Table 1.
Clinical characteristics of deceased donors for pancreas transplantation
※Definition of marginal donor: over 45 years, hemodynamic instability (dopamine < 10 mg/kg/min or use of two or more vasopressors use), or DCD) (Kapur Sandip; Bonham 1999)
※BMI, body mass index; ICU, intensive care unit; HLA, human leukocyte antigen
Recipient-related characteristics
The characteristics of all recipients are summarized in Table 2. The median postoperative observation period was 1968 days (96-8071). The recipients had a median diabetes duration of 25 years and had been on dialysis for 5.1 years. The median post-transplant hospital stay (PTHS) was 56 days.
The median TIT values for the pancreas and kidneys were 604 min and 951 min, respectively. Reconstruction of the GDA and portal vein extension were required in six and two cases, respectively.
Enteric drainage was predominantly performed via duodenoileostomy with side-to-side anastomosis. Enteric drainage was performed using the Roux-en-Y method in a patient with a history of peritonitis due to appendicitis because of the need for partial resection of the ileum.
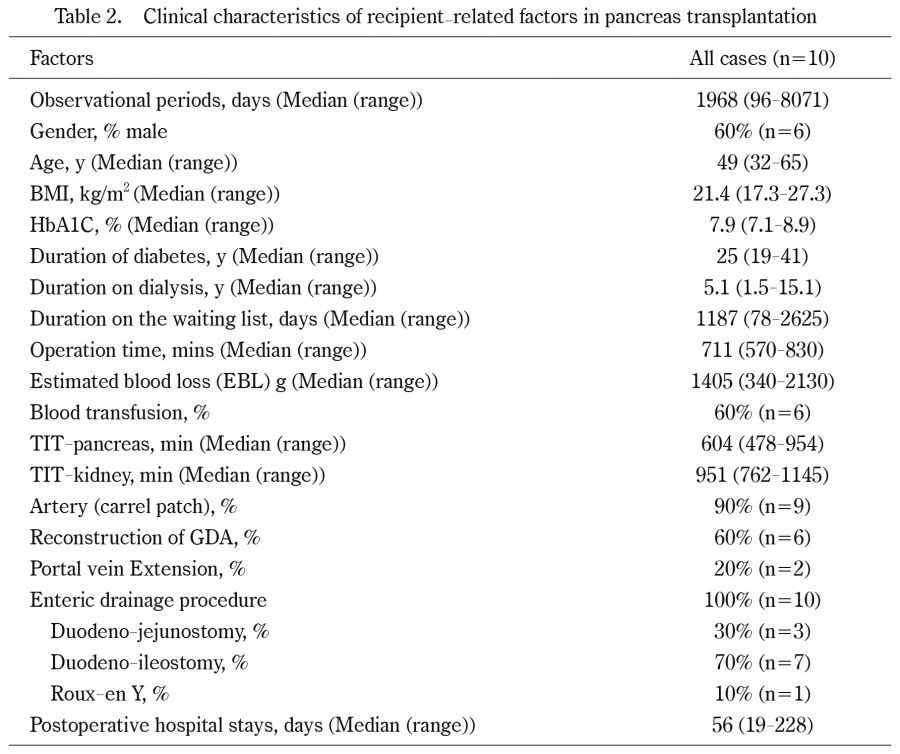
Table 2.
Clinical characteristics of recipient-related factors in pancreas transplantation
BMI, body mass index; TIT, total ischemic time; HBA1c, glycosylated hemoglobin
Postoperative complications of SPK
Postoperative complications were observed in all the patients (Table 3). Most of these complications were classified as Clavien-Dindo (CD) grade I or II. Major complications classified as CD grade IIIa or higher were observed in four patients (40%); however, mortality was zero. Major complications included postoperative bleeding from the kidney graft zero-hour biopsy site, primary nonfunctioning kidney graft, wound dehiscence, and peritonitis due to perforation of the ileal stump after Roux-en-Y anastomosis. The first three major complications were successfully treated with surgical intervention. However, one patient with peritonitis required two additional surgeries and temporary intensive care unit (ICU) management because of sepsis resulting from peritonitis. The cause of the ileal stump perforation was obstruction associated with adhesions of the ileum on the anal side of the anastomosis. However, none of the patients experienced duodenal graft perforation.
The median CCI for all cases was 37.9, and a correlation was observed between the CCI and the PTHS (Fig. 1). An R2 value of 0.5876, corresponding to an R-value of approximately 0.77, suggests a moderate correlation between the CCI and length of postoperative stay. The ten patients were divided into two groups: the early group (2001-2018) and the late group (2019-2024), with five patients in each group. A comparison of CCI between the groups showed a trend toward reduction in the late group compared to the early group (early group:41.8 vs. late group:29.6; p=0.056). (Fig. 2). The median PTHS of all patients was 56 days. However, similar to the trend observed with the CCI, the PTHS tended to be shorter in the late group than in the early group (early group:67 days vs. late group:30 days; p=0.056). We believe that the reduction in the PTHS may be related to a decrease in perioperative complications.
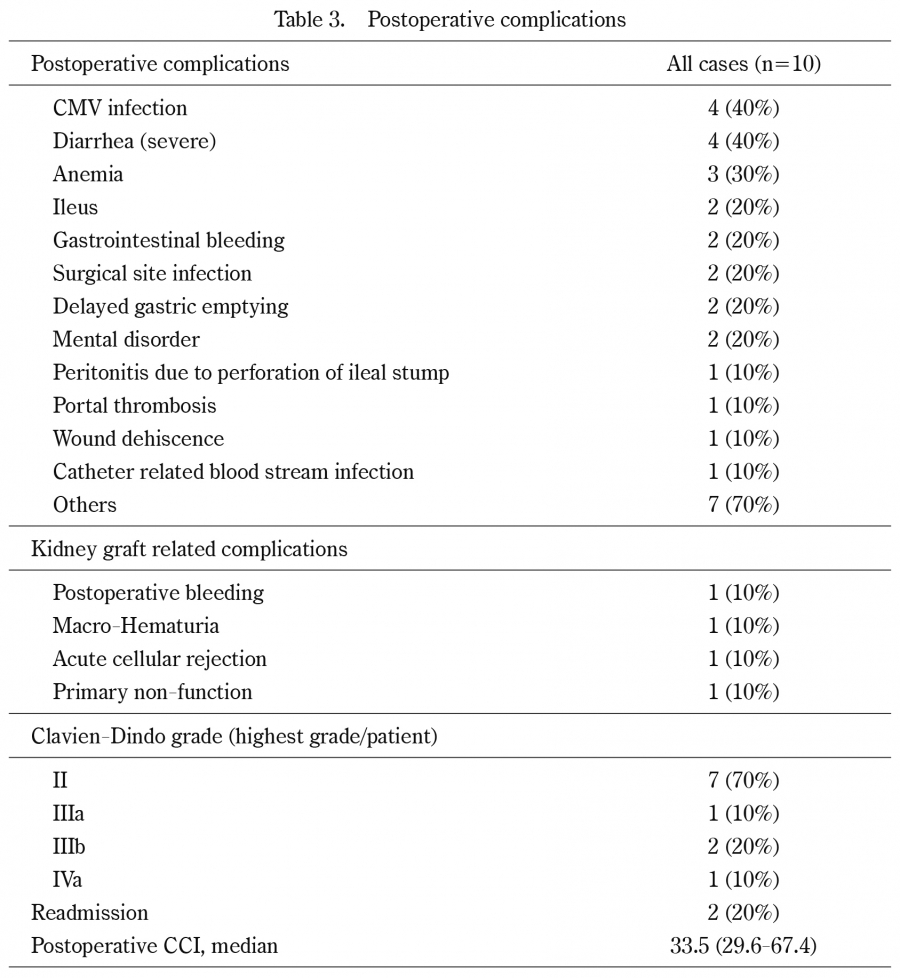
Table 3.
Postoperative complications
Comprehensive complication index (CCI) (Slankamenac K, et al. Ann Surg. 2013; 258(1): 1-7)
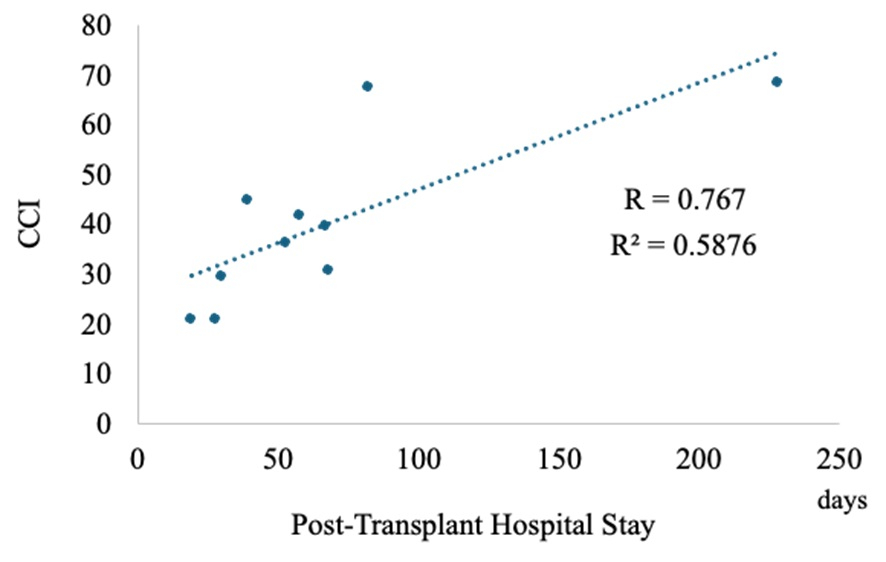
Fig. 1.
Association Between Post-Transplant Hospital Stay and CCI.
A correlation was observed between the CCI and post-transplant hospital stay. An R2 value of 0.5876, corresponding to an R-value of approximately 0.77, suggests a moderate correlation between the CCI and the length of postoperative stay.
CCI, comprehensive complication index.
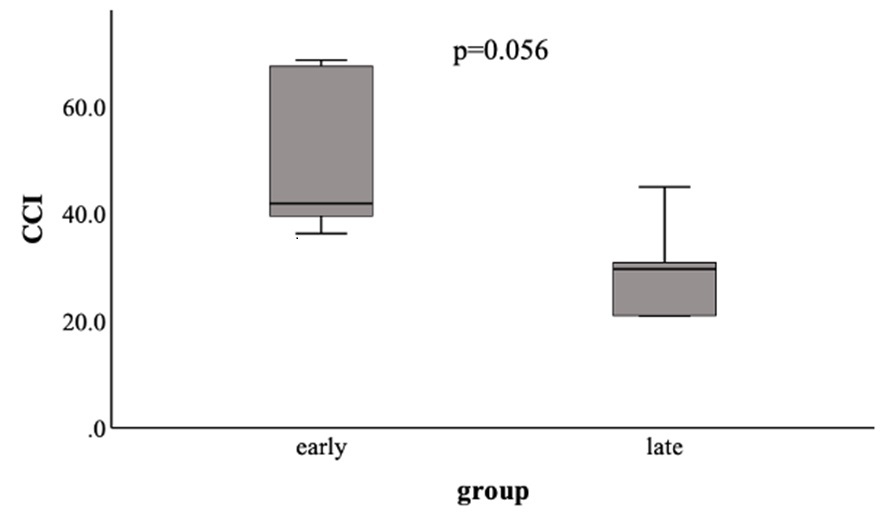
Fig. 2.
Comparison of Mean CCI Values Between Group A and Group B.
The ten patients were divided into two groups:the early group (2001-2018) and the late group (2019-2024), with five patients in each group. A comparison of CCI between the groups revealed a trend toward a decrease in CCI in the late group (early group:41.8 vs. late group:29.6; p=0.056).
CCI, comprehensive complication index.
Outcomes of pancreas transplantation and late-onset complications
Patient, pancreatic, and kidney graft survival rates are shown in Fig. 3. The pancreatic and kidney functions are shown in Figs. 4a and 4b. Despite the loss of one kidney graft due to primary nonfunction, the 5-year outcomes for both patient survival and pancreatic graft survival remained 100%. However, we encountered one case each of pancreatic graft loss, kidney graft loss, and patient death, all of which were attributed to LOC.
Among the 10 cases, six LOCs were observed in five cases. LOC onset occurred between one- and 16-years post-transplant. One patient with acute pancreatitis was treated with medication. Two patients required reoperation because of incisional hernia and strangulation of the bowel obstruction. One patient developed hyperglycemic acidosis and resumed insulin therapy 5 years post-transplantation. Although histological confirmation was not obtained, the patient was diagnosed with recurrent T1DM based on blood tests (no elevation of serum amylase and lipase levels), seroconversion of the anti-IA-2 antibody, and imaging findings (no graft pancreatitis or thrombosis). A case of kidney graft loss 6 years post-transplantation resulted from the progression of focal segmental glomerulosclerosis (FSGS). One patient suddenly died of cardiovascular disease 8 years after undergoing SPK with a functioning graft.
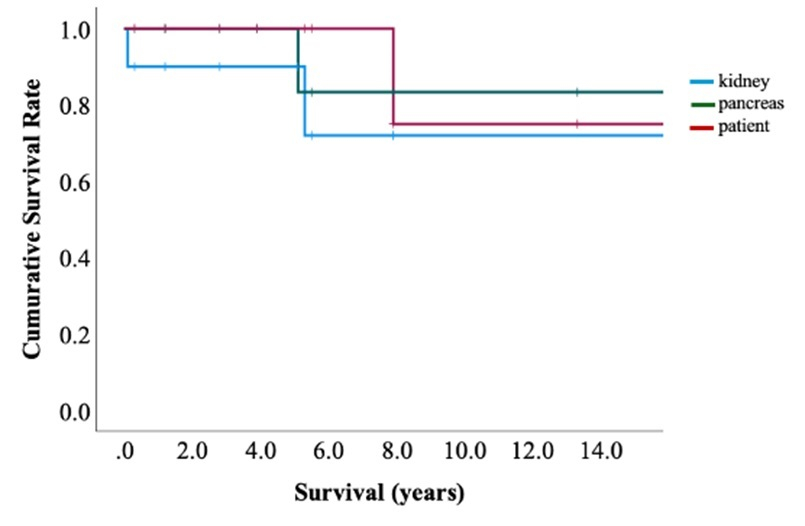
Fig. 3.
Patient Survival Rate, Pancreas Graft Survival Rate, and Kidney graft Survival Rate.
Patient, pancreatic, and kidney graft survival rates are shown. Despite the loss of one kidney graft due to primary nonfunction, the 5-year outcomes for both patient and pancreatic graft survival remained 100%. However, we encountered one case each of pancreatic graft loss, kidney graft loss, and patient death after 5 years post-transplantation, all of which were attributed to LOC.
LOC, late-onset complications.
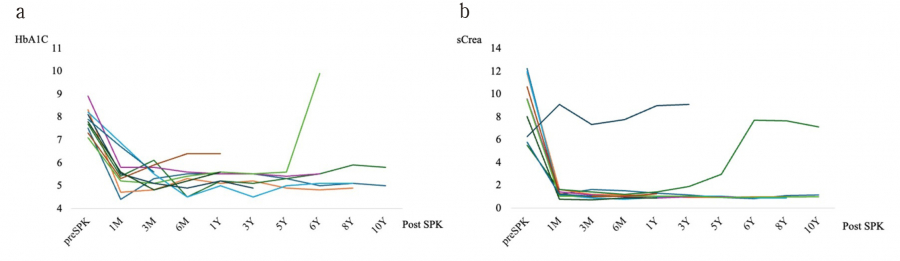
Fig. 4.
Time Course of HbA1C (a) and sCrea (b).
The HbA1c level was maintained below 6.1% at 3M after SPK. HbA1c was elevated in one case due to recurrence of T1MD after 5-year SPK. All but one primary nonfunction kidney patient achieved a hemodialysis-free condition after SPK and maintained a sCrea level below 2.0 mg/dL for 3 years after SPK. One patient required hemodialysis because of end-stage renal disease caused by FSGS.
LOC, late-onset complications; SPK, simultaneous pancreas-kidney transplantation; FSGS, focal segmental glomerulosclerosis.

