Therapeutic Agents and Patient Characteristics Affecting Metabolism of Thiopurines in Patients with Inflammatory Bowel Disease
Masato Aizawa, Kohei Suzuki, Yuki Nakajima, Kenichi Utano, Kana Tamazawa, Kenta Ueda, Jun Wada, Kentaro Sato, Goro Shibukawa, Noriko Tanaka, Kazutomo Togashi
Author information
- Masato Aizawa
Department of Coloproctology and Gastroenterology, Aizu Medical Center Fukushima Medical University - Kohei Suzuki
Department of Coloproctology and Gastroenterology, Aizu Medical Center Fukushima Medical University - Yuki Nakajima
Department of Coloproctology and Gastroenterology, Aizu Medical Center Fukushima Medical University - Kenichi Utano
Department of Coloproctology and Gastroenterology, Aizu Medical Center Fukushima Medical University - Kana Tamazawa
Department of Coloproctology and Gastroenterology, Aizu Medical Center Fukushima Medical University - Kenta Ueda
Department of Coloproctology and Gastroenterology, Aizu Medical Center Fukushima Medical University - Jun Wada
Department of Coloproctology and Gastroenterology, Aizu Medical Center Fukushima Medical University - Kentaro Sato
Department of Coloproctology and Gastroenterology, Aizu Medical Center Fukushima Medical University - Goro Shibukawa
Department of Coloproctology and Gastroenterology, Aizu Medical Center Fukushima Medical University - Noriko Tanaka
Health Data Science Research Section, Tokyo Metropolitan Institute of Gerontology
Clinical Research Center, Fukushima Medical University Hospital, Fukushima Medical University - Kazutomo Togashi
Department of Coloproctology and Gastroenterology, Aizu Medical Center Fukushima Medical University
Introdution
In inflammatory bowel disease (IBD), including ulcerative colitis (UC) and Crohn’s disease (CD), a chronic inflammatory disorder of the intestinal mucosa causes repeated relapses and remissions, leading to the gradual accumulation of intestinal damage1). Prompt induction of remission and its sustained maintenance are essential treatment strategies to eliminate intestinal damage2, 3). Recent advancements in IBD treatment have been significant, though thiopurines remain key drugs4, 5). Thiopurines were originally developed as therapeutic agents for childhood leukemia6), and their immunomodulatory effects on IBD were initially reported in the late 1960s 7). Currently, thiopurines are used to maintain long-term, steroid-free remission and to prevent secondary failure of anti-tumor necrosis factor αagents in IBD patients8, 9).
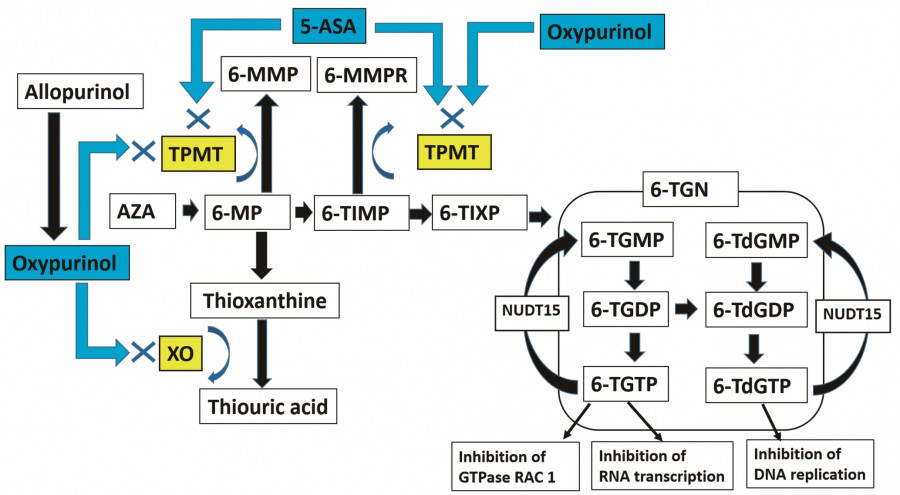
Several enzymes are involved in the metabolism of thiopurines, including azathioprine (AZA) and 6-mercaptopurine (6-MP), and these metabolic enzymes can be affected by various agents, as illustrated in Figure 1. It is well known that two key drugs used in the treatment of IBD patients affect thiopurine metabolism10, 11). The first one is allopurinol, a uric acid synthesis inhibitor, which is metabolized to oxypurinol. Allopurinol exerts its effect on thiopurine metabolism by inhibiting both xanthine oxidase (XO) and thiopurine S-methyltransferase (TPMT)12). Through these two different pathways, allopurinol strongly increases the levels of 6-TGN, which is significantly and independently associated with the therapeutic response in IBD13). The second drug is 5-aminosalicylic acid (5-ASA), which interacts with thiopurine metabolism by inhibiting TPMT14). However, the effect of 5-ASA on thiopurine metabolism varies depending on the specific formulation, and the administration of time-dependent 5-ASA alone can impact thiopurine metabolism15).
Apart from allopurinol and time-dependent 5-ASA, limited reports have examined the factors affecting the metabolism of thiopurines in real-world settings16,17). Furthermore, few reports have clarified the relationships between the concentrations of thiopurine metabolites and sex, age, NUDT15 (nucleoside diphosphate-linked moiety X-type motif 15), etc. This study focused on the intracellular concentrations of 6-TGN and 6-MMP associated with hepatoxicity and investigated the effects of concurrent medications and patient characteristics on the intracellular concentrations of 6-TGN and 6-MMP in IBD patients undergoing thiopurine therapy.
Methods
Study design
This was a single-center, retrospective, observational study. Before the study commencement, the Institutional Review Board of Fukushima Medical University approved the study and waived the requirement for informed consent (Registration No. General 2021-212). All data were collected by December 2022. The Strengthening the Reporting of Observational Studies guidelines were followed in reporting this study.
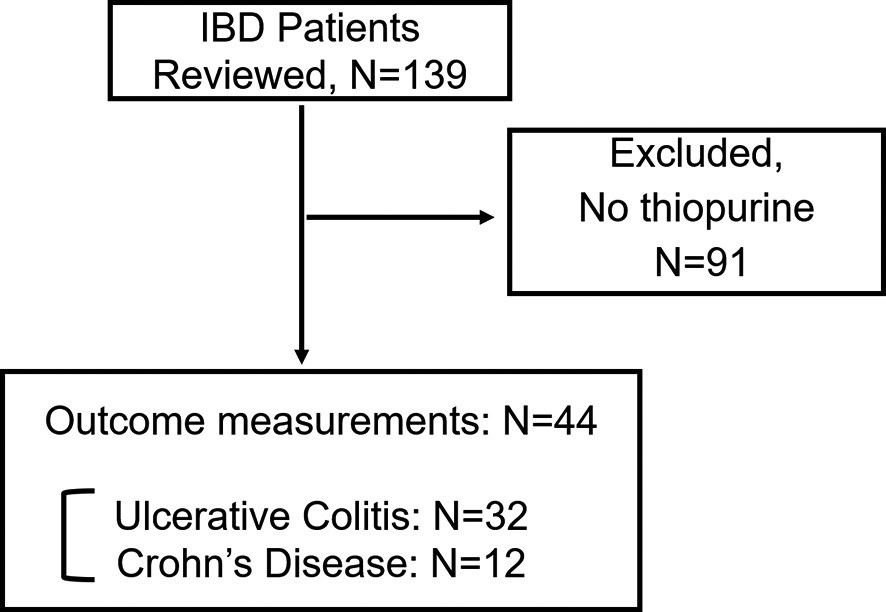
Study Flow (Figure 2)
Of the 139 IBD patients who visited the Aizu Medical Center between May 2013 and October 2021, 44 patients (32 with UC, 12 with CD) who received thiopurine treatment and underwent 6-TGN and 6-MMP concentration measurements were included in the study (Figure 2). Relevant information, including short-term outcomes, was extracted from medical records. The intracellular concentrations of 6-TGN (therapeutic range:235-450 pmol/8 × 108RBC) and 6-MMP (addiction level:≥ 5,700 pmol/8 × 108RBC), were measured by the LSI Medience Corporation (Tokyo, Japan) using liquid chromatography-tandem mass spectrometry (LC -MS/MS). The 6-TGN concentrations in RBCs were measured Before starting thiopurine administration, the presence of NUDT15 polymorphism, which affects thiopurine metabolism and can lead to severe hematological toxicity in patients with the genetic variant, was primarily investigated. The dose of thiopurine was adjusted to a smaller dose, particularly at the time of initial prescription, to account for the risk of leukopenia in heterozygous patients. Disease activity was assessed using the partial-Mayo score (p-Mayo) for UC and the Crohn’s Disease Activity Index (CDAI) for CD. Disease activity was categorized as “mild” (p-Mayo score ≤ 3, CDAI ≤ 220), “moderate” (4 ≤ p-Mayo score ≤ 6, 221 ≤ CDAI ≤ 450), or “severe” (p-Mayo score > 6, CDAI > 450). The dose of AZA (mg) in 6-MP was calculated with the conversion formula of 2.08× 6-MP (mg)18).
Outcome Measures
The initial measurement of 6-TGN and 6-MMP levels was conducted 3±1 months after initiating thiopurine administration, and the initial measurement of each patient was used for this study. The primary outcome measure was to investigate factors affecting 6-TGN levels, including patient background factors such as age, sex, UC or CD diagnosis, disease activity, and NUDT15 polymorphism, as well as concomitant therapeutic agents (thiopurine dose and formulation, 5-ASA dose and formulation, steroids, biologics, and allopurinol). The secondary outcome measure was to investigate factors affecting 6-MMP levels and adverse events. In addition, the 5-ASA formulation was categorized into time-dependent 5-ASA and other types of 5-ASA (pH-dependent, multimatrix, salazosulfapyridine) and investigated the effect of time-dependent 5-ASA on 6-TGN and 6-MMP levels, because time-dependent 5-ASA can be absorbed in the small intestine and inhibit TMPT activity in the blood.
Statistical Methods
Patients’ characteristics are reported as descriptive statistics, with continuous variables expressed as median and interquartile range (IQR) values and categorical variables expressed as counts and percentages. Continuous variables were compared using the Mann-Whitney U test, and categorical variables were compared by Fisher’s exact test. Furthermore, a one-way analysis of variance (ANOVA) was performed, taking into consideration the normal distribution exhibited by the logarithmically transformed 6-TGN/6-MMP levels. Subsequently, multivariate ANOVA was performed, incorporating variables with a significance level set at p < 0.2. The normality of the distribution was assessed by the Shapiro-Wilk W test. All p values are two-tailed, and values < 0.05 were considered significant. All statistical analyses were performed with Stata 16.1 (Stata Corp, College Station, Texas, USA).
Results
Patients’ Characteristics (Table 1)
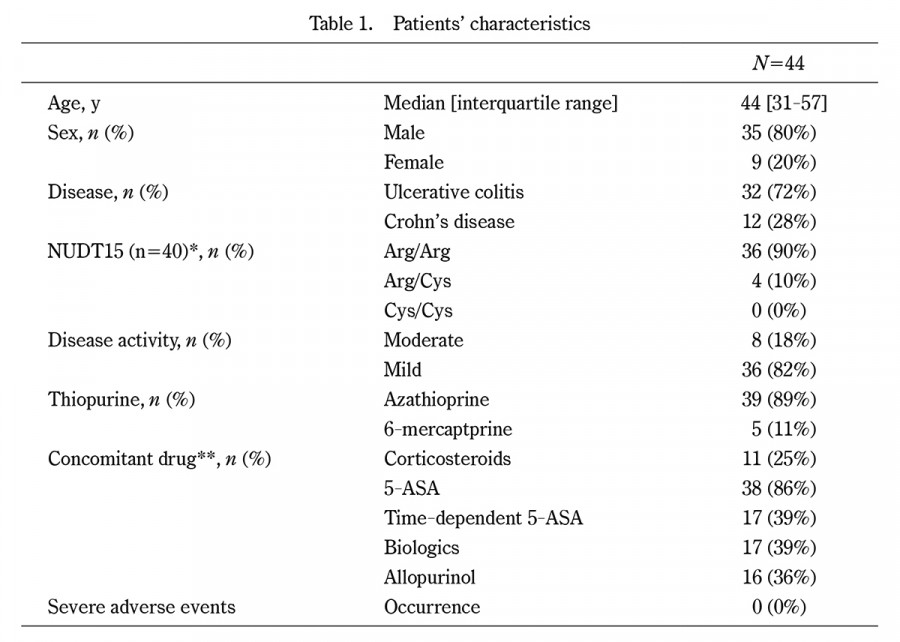
A total of 44 IBD patients (35 males, 9 females), with a median age of 44 years, were included in the study. Of these patients, 32 had UC and 12 had CD. NUDT15 polymorphism was measured in 40, and the NUDT15 variants showed a prevalence of 10%, with 4 patients having the Arg/Cys variant and none having the Cys/Cys variant. Regarding disease activity, 82% of patients had mild activity, 18% had moderate activity, and none had severe activity. In addition, all patients with CD showed mild activity. Most patients underwent administration of AZA (89%) as thiopurine and 5-ASA (86%) as concomitant drugs. No severe adverse events, including severe hematological toxicity and alopecia, were observed during the study period.
Factors affecting 6-TGN and 6-MMP levels
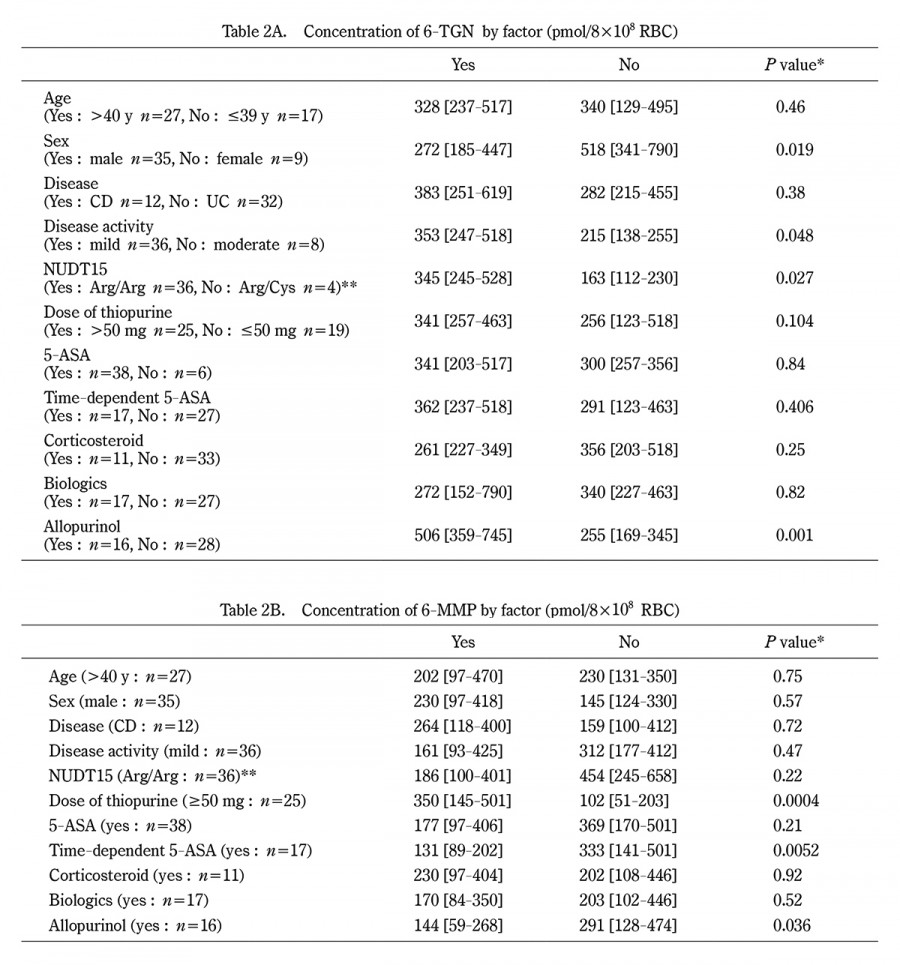
As shown in Table 2A, the 6-TGN levels showed significant differences by sex (p=0.019), disease activity (p=0.048), and NUDT15 polymorphism (p=0.027). In terms of concomitant agents, there was a significant increase in patients who were administered allopurinol (p=0.001) and a trend toward an increase in patients receiving high-dose thiopurine treatment (p=0.104).
The 6-MMP levels did not show any significant differences in patients’ characteristics, as shown in Table 2B. Nonetheless, significant increases were observed in patients who underwent high-dose thiopurine treatment (p=0.0004) and in those who did not receive time-dependent 5-ASA (p=0.0052) or allopurinol (p=0.036).
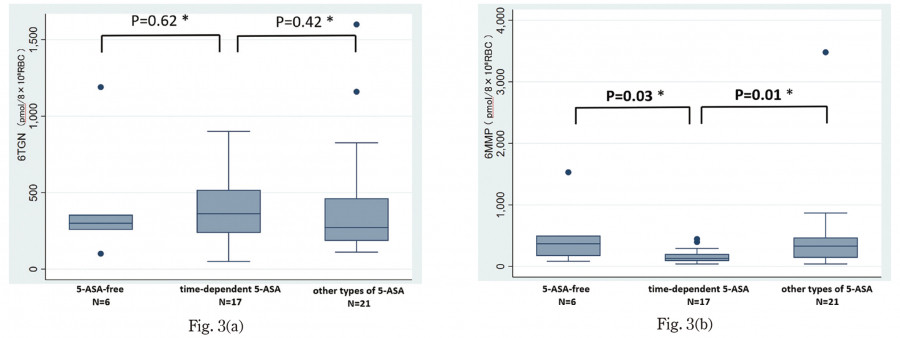
Effect of 5-ASA Formulations on 6-TGN and 6-MMP Levels
The levels of 6-TGN were 300 [interquartile range 257-356] pmol/8 × 108 RBC in the 5-ASA-free group, 362 [237-518] pmol/8 × 108 RBC in the time-dependent 5-ASA group, and 272 [185-463] pmol/8 × 108 RBC in the other types of 5-ASA group, as shown in Figure 3(a). However, no significant differences were observed in any of the comparisons made. In contrast, 6-MMP levels were 369 [170-501] pmol/8 × 108 RBC in the 5-ASA-free group, 131 [89-202] pmol/8 × 108 RBC in the time-dependent 5-ASA group, and 330 [141-470] pmol/8 × 108 RBC in the other types of 5-ASA group. Significant differences were found between the time-dependent 5-ASA group and the 5-ASA-free group (p=0.035), as well as between the time-dependent 5-ASA group and the other types of 5-ASA group (p=0.011), as shown in Figure 3(b).
Factors Affecting Logarithmically Transformed 6-TGN and 6-MMP Levels
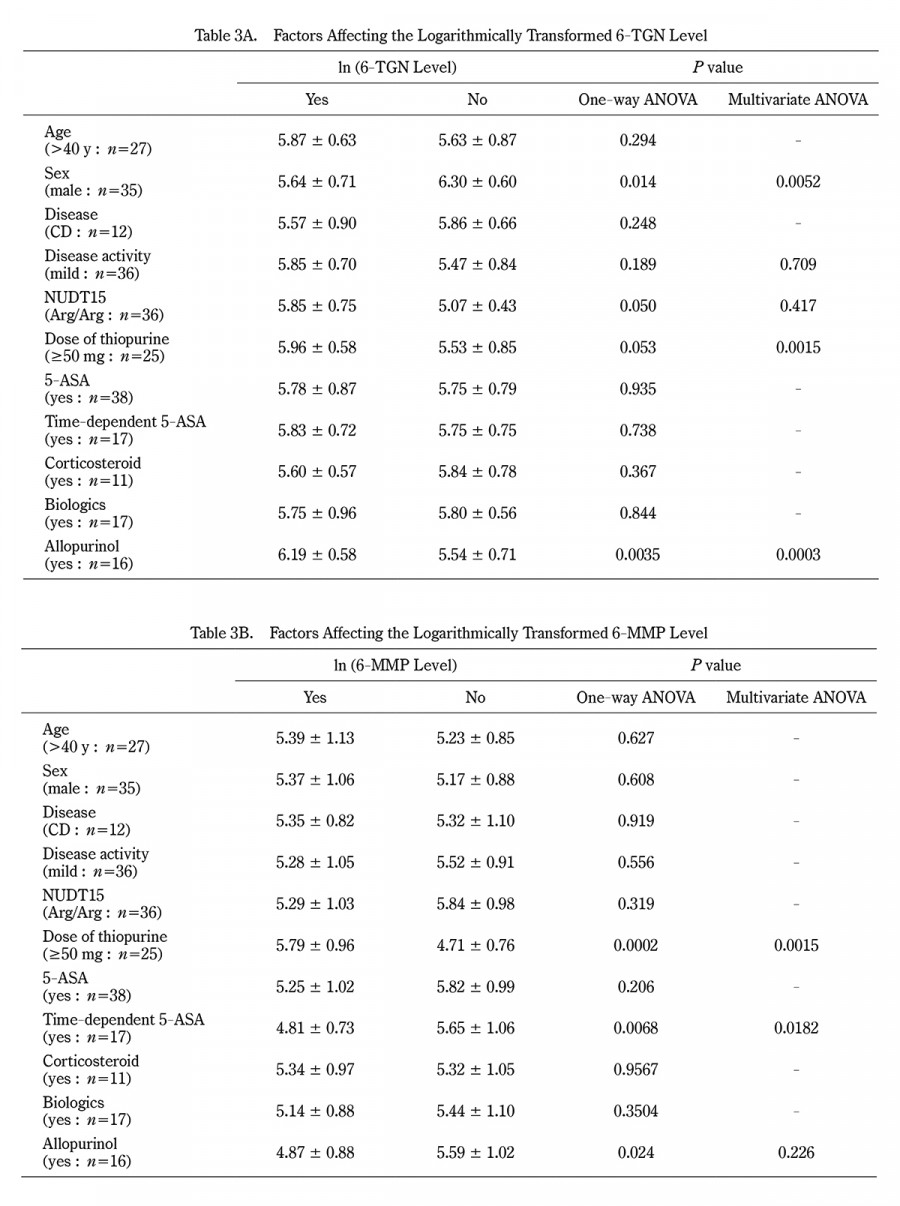
The 6-TNG levels followed a normal distribution after logarithmic transformation (Shapiro-Wilk W test, p = 0.938). One-way ANOVA identified significant differences by sex (p = 0.0141) and administration of allopurinol (p = 0.0035). Factors such as disease activity (p = 0.189), NUDT15 polymorphism (p = 0.0503), and thiopurine dose (p = 0.0529) were associated with 6-TGN levels. On multivariate ANOVA with these covariates, sex (p = 0.0052), thiopurine dose (p = 0.0015), and administration of allopurinol (p = 0.0003) showed significant associations with the logarithmically transformed 6-TGN level, as shown in Table 3A.
Similarly, the logarithmically transformed 6-MMP levels showed a normal distribution (Shapiro-Wilk W test, p = 0.348). One-way ANOVA identified significant differences based on thiopurine dose (p = 0.0002), time-dependent 5-ASA (p = 0.0068), and allopurinol (p = 0.024). On multivariate ANOVA with those covariates, only the thiopurine dose showed a significant difference (p = 0.0015), as shown in Table 3B.
Discussion
This study investigated factors affecting intracellular 6-TGN and 6-MMP levels in IBD patients and confirmed the effects of allopurinol, thiopurine dosage, and time-dependent 5-ASA in a real-world setting. Administration of corticosteroids and biologics did not show any significant effects on 6-TGN and 6-MMP levels. As for patient factors, 6-TGN levels were affected by sex, disease activity, and status of NUDT15 polymorphism on univariate analysis, and sex alone significantly affected 6-TGN levels on multivariate ANOVA. In contrast, no patient factors affected 6-MMP levels.
Administration of allopurinol had a significant effect on 6-TGN and 6-MMP levels, except on multivariate ANOVA. This may be attributed to the double inhibitory action on XO and TPMT12). This action reduces hepatotoxicity caused by 6-MMP and can also enhance the efficacy of thiopurine by increasing 6-TGN levels, even with a small amount of thiopurine. In fact, the therapeutic efficacy for mucosal healing and safety of low-dose thiopurine in combination with allopurinol has been reported in recent years19).
The dose of thiopurine affected both 6-TGN and 6-MMP levels, with higher 6-TGN levels observed in females. Since women generally tend to have smaller physiques than men, this observation may seem obvious. Nevertheless, clinicians should still be aware of these findings when prescribing thiopurine. In addition, 6-MMP can be greatly affected by thiopurine dose because 6-MMP is generated in the early phase of thiopurine metabolism.
Previous reports demonstrated that 6-TGN levels increased significantly in CD patients who received thiopurine with 5-ASA compared to those who did not14). Morikubo et al. examined 6-TGN levels with different 5-ASA types and reported a significant concentration increase of 6-TGN with time-dependent 5-ASA. This mechanism is thought to involve the fact that a large proportion of time-dependent 5-ASA is absorbed in the epithelium of the small intestine and inhibits TPMT activity15). In the present study, however, administration of time-dependent 5-ASA decreased 6-MMP levels, but it did not significantly increase 6-TGN levels. This inconsistency may be related to less statistical power due to the small sample size.
As for patient background, a significant increase in 6-TGN levels was observed in patients with mild disease activity compared with moderate cases. This suggests that disease activity could be controlled in patients with high 6-TGN levels. Indeed, Hanai et al. reported that 6-TGN levels in UC patients were significantly lower in the relapse group20). Generally, thiopurine is not used in both UC and CD with severe disease activity because it takes approximately two months for the effect of thiopurine to manifest. In addition, no patients with severe disease activity received thiopurine in the present study.
NUDT15 is a gene involved in the metabolism of 6-TGN. One percent of Asians have a homozygous gene mutation, and severe side effects such as severe leukopenia and alopecia can be seen21). Therefore, the identification of NUDT15 genetic mutations is essential for Asian patients. Theoretically, its genetic polymorphism does not change the total amount of 6-TGN, but it alters the proportion of 6-TGMP (6-thio-guanosine monophosphate), 6-TGDP (6-thio-guanosine diphosphate), and 6-TGTP (6-thio-guanosine triphosphate), all in the 6-TGN family22). In the present study, 6-TGN concentrations were lower in heterozygous patients. A plausible explanation is that the dose of thiopurine was lowered to a smaller dose, particularly at the time of initial prescription, to account for the risk of leukopenia in heterozygous patients, although this tendency was not clear in the present study.
This study has several limitations. First, this was a retrospective study conducted in a single hospital and subject to selection bias. Second, the number of patients examined was relatively small. With a small sample size, the possibility of committing a Type II error (β), which is judged as no significant difference when in fact there is a significant difference, must always be considered. Indeed, the administration of time-dependent ASA did not affect 6-TGN levels in this study. Third, only 6-TGN and 6-MMP levels were measured of the various thiopurine metabolites. For instance, 6-MMPR (6-methylmercaptopurine ribonucleotide), which is generated during the metabolic process of 6-MP and may cause liver damage, was not at all investigated. Other thiopurine metabolites might be measured to further elucidate thiopurine metabolism in a future study.
In conclusion, patients who received allopurinol, a high dose of thiopurine, or were female exhibited higher 6-TGN levels in a real-world setting. Patients who received high-dose thiopurine had higher 6-MMP levels, but those given allopurinol or time-dependent 5-ASA had lower 6-MMP levels. Clinicians should take note of these findings that 6-TGN and 6-MMP concentrations were affected by patient background factors, including NUDT15 gene polymorphism, and concomitant drugs when prescribing thiopurine.
Conflict of Interest
The authors have no competing interests to disclose.
Acknowledgment
The authors thank FORTE Science Communications (https://www.forte-science.co.jp/) for editing the English language of this manuscript.
Ethics approval and consent to participate
Approval for a waiver of informed consent was obtained from the Institutional Review Board of Fukushima Medical University (Registration No. 2021-212).
Authors’ Contributions
Masato Aizawa and Kazutomo Togashi wrote the main document. Masato Aizawa, Kazutomo Togashi, Kohei Suzuki, Yuki Nakajima and Kenichi Utano substantially contributed to the conception of the work. Masato Aizawa, Kazutomo Togashi, Kohei Suzuki, Yuki Nakajima and Kenichi Utano, Kana Tamazawa, Kenta Ueda, Jun Wada, Kentaro Sato, and Goro Shibukawa contributed to the acquisition of data. Masato Aizawa, Kazutomo Togashi and Noriko Suzuki contributed to the interpretation of data. All authors reviewed the manuscript.
Data Availability
The raw data used in this study are available upon request from the corresponding author for replication and verification.
Abbreviations
IBD:inflammatory bowel disease
UC:ulcerative colitis
CD:Crohn’s disease
5-ASA:5-aminosalicylic acid
AZA:azathioprine
6-MP:6-mercaptopurine
6-TGN:6-thioguanine nucleotide
6-TIMP:6-thio-inosine monophosphate
6-TXMP:6-thio-xanthosine monophosphate
6-MMP:6-methylmercaptopurine
6-MMPR:6-methylmercaptopurine ribonucleotide
6-TGMP:6-thio-guanosine monophosphate
6-TGDP:6-thio-guanosine diphosphate
6-TGTP:6-thio-guanosine triphosphate
6-TdGMP:6-thio-deoxyguanosine monophosphate
6-TdGDP:6-thio-deoxyguanosine diphosphate
6-TdGTP:6-thio-deoxyguanosine triphosphate
TPMT:Thiopurine S-methyltransferase
NUDT15:Nucleoside diphosphate-linked moiety X-type motif 15
p-Mayo:partial-Mayo score
CDAI:Crohn’s disease activity index
IQR:interquartile rage
ANOVA:analysis of variance
XO:xanthine oxidase