Community-based rehabilitation (CBR) aims to enable older adults with disabilities and their families to continue living in their own homes1) CBR is categorized into home-visit rehabilitation, in which therapists visit patients, and outpatient rehabilitation, in which patients visit facilities for treatment2) Adequate access to rehabilitative treatment is important for preventive care, maintenance of physical and mental functions, and enabling patients to live in their preferred community.
Both patient-related and circumstantial factors affect access to CBR. Patient-related factors, including the aging process itself, fracture, and dementia, commonly cause increased long-term care needs3) Additionally, circumstances related to geographical distance and lack of healthcare resources in rural areas affect rehabilitation access4-6)
Nuclear disasters significantly complicate CBR access. In addition to circumstantial difficulties, evacuation and repopulation contribute to the aging of the area’s population and reduced social interaction7,8) Several studies have reported on medical care provision in communities after nuclear disasters9-14) Although few, these reports have emphasized the importance of securing CBR in resource-scarce areas.
In 2011, the Great East Japan Earthquake and resulting tsunami caused the Fukushima Daiichi Nuclear Power Plant (FDNPP) accident. Examining CBR in the resource-scarce areas repopulated following this disaster is essential. Kawauchi Village in Fukushima Prefecture is a rural, mountainous area located 10-30 kilometers southwest of the FDNPP and was an evacuation zone after the accident (Figure 1)15) After 10 years, approximately 2000 of the 2800 former residents have already repopulated the village. However, there are still post-disaster effects due to the prolonged nuclear disaster circumstances, such as a lack of social resources and changes in the family structure and neighborhoods. Although the area has one clinic, there are no rehabilitation facilities. Despite some residents seeking rehabilitation care, securing specialized medical personnel to provide treatment in rural and remote areas is difficult5)
Given these circumstances, various efforts have been made to deliver CBR to Kawauchi Village, including those of Healthcare Corporation Seireikai in Hirata Village, which provides home-visit rehabilitation care16) However, little information is available on facility-based rehabilitation services for people in the former evacuation zone.
Herein, we present an older couple living in Kawauchi Village who required rehabilitation care. This case report may provide insight into the post-disaster provision of CBR in resource-scarce areas.
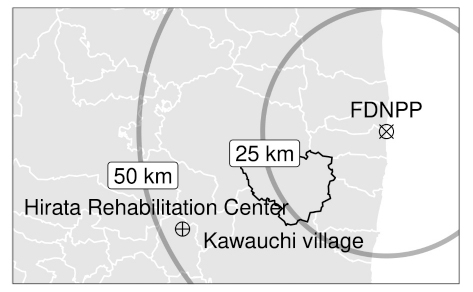
Fig. 1. Geographical locations of Kawauchi Village, Hirata Rehabilitation Care Center, and Fukushima Daiichi Nuclear Power Plant (FDNPP).