

Pseudomyxoma peritonei (PMP) is a rare disease, with an estimated incidence of approximately 1-2 cases per million1,2), that is often associated with peritonitis carcinomatosa caused by accumulated mucus. It often has a clinically malignant course, but in recent years aggressive cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) have led to a dramatic improvement in prognosis1). In this article, we present four cases of PMP diagnosed as a result of giant ovarian tumors at our hospital, and discuss the epidemiology, classification, diagnosis, recent multidisciplinary treatment, and prognosis of PMP in the literature.
The content of research paper
Four cases of pseudomyxoma peritonei with ovarian tumors at our hospital
Riho Yazawa, Hiroyuki Yazawa, Kaoru Fukuda, Miki Ohara, Fumihiko Osuka
Author information
-
Riho Yazawa
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
-
Hiroyuki Yazawa
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
-
Kaoru Fukuda
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
-
Miki Ohara
Department of Obstetrics and Gynecology, Fukushima Red Cross Hospital
-
Fumihiko Osuka
Department of Surgery, Fukushima Red Cross Hospital
Introduction
Cases
Cases 1 and 2 were previously reported in 20203), and their courses are described briefly here.
Case 1: A 26-year-old woman with a giant abdominal tumor was referred to our department in 2007. She was diagnosed with a large multicystic ovarian tumor and massive ascites based on magnetic resonance imaging (MRI) (Fig. 1A) and computed tomography (CT) (Fig. 1B). Laparotomy was performed. A tumor in the left ovary had ruptured, leading to massive gelatinous mucinous ascites (Fig. 1C). Left adenectomy and appendectomy were performed. The postoperative pathological diagnosis was mucinous borderline tumor of the ovary (Fig. 1D). No tumor was detected in the appendix (Fig. 1E), leading to a diagnosis of PMP originating from a borderline ovarian tumor. The patient was treated with fertility-preserving staging laparotomy and three courses of intraperitoneal chemotherapy. There has been no recurrence in the 15 years since her first operation.
Case 2: A 72-year-old woman with abdominal distension was referred to our department due to a giant abdominal tumor detected by MRI and CT in 2018 (Fig. 2A,B). Laparotomy was performed. A tumor in the left ovary had ruptured and there was gelatinous mucinous ascites throughout the abdominal cavity (Fig. 2C). Bilateral adenectomy, partial omentectomy, and appendectomy were performed (Fig. 2D). The postoperative pathological diagnosis revealed low-grade appendiceal mucinous neoplasm (LAMN) (Fig. 2E) and mucinous cystadenoma of the ovary. The patient was diagnosed with PMP originating from LAMN based on immunohistochemical findings (Fig. 3, Table 1). Because she declined standard treatments for PMP, such as aggressive CRS and HIPEC, she was kept under observation. Four months after the first operation, the pelvic peritoneal mucinous tumor recurred. Tumor resection and active lavage with heated saline were performed laparoscopically. The patient has remained asymptomatic with a small amount of ascites for 3 years.
Case 3: An 82-year-old woman with abdominal distention was referred to our department due to a giant ovarian tumor and massive ascites detected by MRI and CT in 2019 (Fig. 4A, 4B). The patient was suspected to have a malignant tumor. An ascites puncture was performed but the fluid was gelatinous, making drainage difficult. The cytological diagnosis of ascites was class III. The patient was diagnosed with PMP based on the nature of the ascites. Although informed consent was obtained regarding treatment, she did not desire treatment at that time and was kept under observation. She was again admitted to the hospital with an acute abdomen, diagnosed with perforation of the gastrointestinal tract and generalized peritonitis (panperitonitis), and underwent emergency laparotomy (Fig. 4C). The diagnosis was perforation of the appendix (Fig. 4D, 4E), and she underwent partial cecal resection and bilateral adnexectomy. The postoperative pathological diagnosis revealed LAMN (Fig. 4F) and mucinous cystadenoma of the ovary. Immunohistochemical staining showed CK7-, CK20+, and CDX2+ in both the appendix and ovaries (Fig. 3, Table 1), leading to a diagnosis of LAMN-derived PMP. Postoperatively, the patient continued to have a small amount of ascites without abdominal symptoms and was transitioned to palliative care.
Case 4: A 48-year-old woman was referred to our department in 2021 because of abdominal distention, ascites, and an ovarian tumor. MRI and CT showed a 14×9 cm multicystic ovarian tumor (Fig. 5A, 5B), with no obvious findings in the appendix. An ascites puncture was performed but the fluid was gelatinous and drainage was difficult. The cytological diagnosis was non-malignant ascites. As a result, PMP was diagnosed, and the patient underwent an emergency laparotomy due to persistent abdominal distention. There was a 3100-ml accumulation of jelly-like ascites, and the left ovarian mucinous tumor had ruptured (Fig. 5C). The appendix was slightly swollen and ruptured (Fig. 5D). Total hysterectomy, bilateral adnexectomy, partial omentectomy, and appendectomy were performed (Fig. 5E). The postoperative pathological diagnosis revealed LAMN (Fig. 5F) and mucinous cystadenoma of the ovary. Based on immunohistochemical findings, the patient was diagnosed with PMP originating from LAMN (Fig. 3, Table 1). Postoperatively, the patient was managed by the surgery department. After informed consent regarding multidisciplinary treatment was obtained, the patient was referred to a specialized facility outside the prefecture, where CRS (resection of the remnant greater mesentery, spleen, lesser mesentery, gallbladder, cecum, inferior diaphragm peritoneum, hepatic peritoneum, abdominal wall peritoneum, etc.) +HIPEC (mitomycin C, 42°C, 1 hour) was performed. Her postoperative course was good and she was discharged 16 days postoperatively. She has been doing well in the 4 months since the multidisciplinary treatment.
Table 1 shows a summary of the four PMP cases. The tumor markers CA125 and CEA were elevated in all cases, but CA199 was elevated only in case 1. In cases 2-4, intraoperative findings showed an enlarged or ruptured appendix, although this was apparent on preoperative imaging studies only in case 2. For all four cases, the PMP classification and the completeness of cytoreduction score (CC score) are shown in the table.
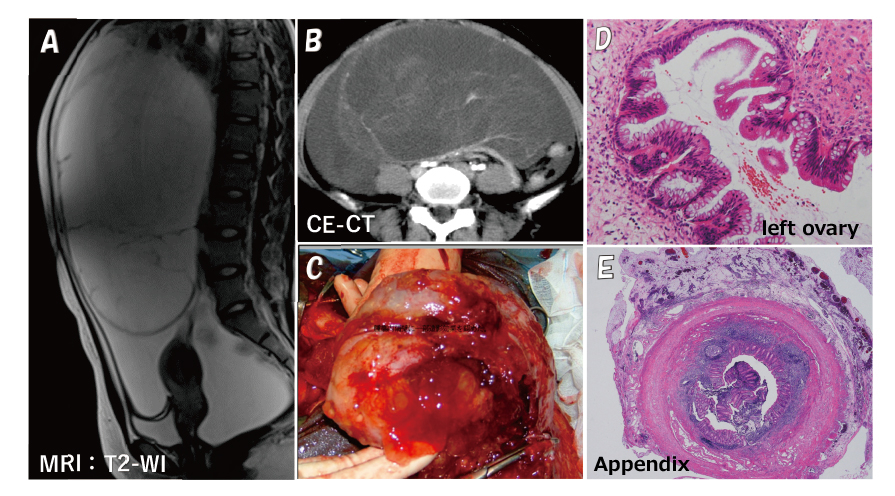
Fig. 1. MRI and CT results, and operative and histopathological findings in Case 1
A T2-weighted sagittal MRI image shows a multicystic ovarian tumor with a diameter of >20 cm and accumulation of massive ascites (A). Contrast-enhanced CT shows a contrast effect on the septum of a giant ovarian tumor (B). The tumor was partially ruptured, leaking and filling the abdominal cavity with jelly-like mucinous contents (C). The ovarian tumor was diagnosed as a mucinous borderline tumor with no noticeable cellular atypia, although some cysts showed protrusion of the epithelium into the lumen and cellular multilayering, and the appearance of island-like free cell masses in some cysts (D). The appendix exhibits massive mucus deposits on the serosal surface, but no neoplastic growths on the mucosal side of the lumen (E).
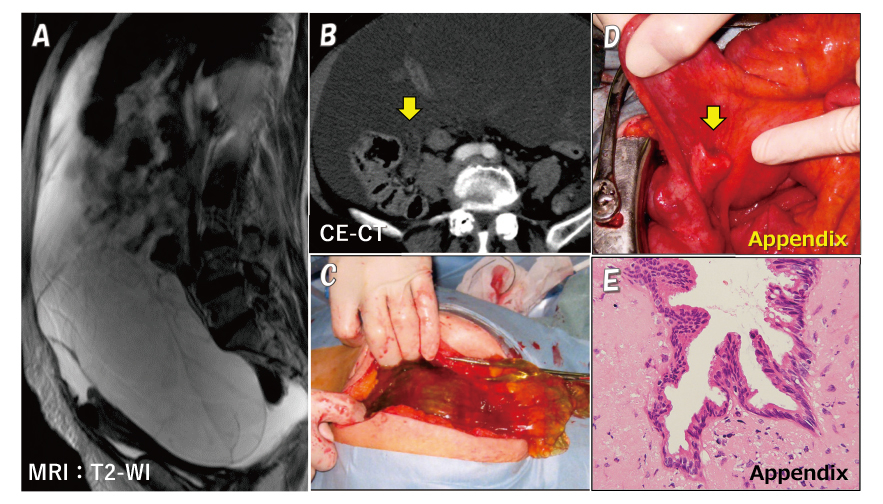
Fig. 1. MRI and CT results, and operative and histopathological findings in Case 1
A T2-weighted sagittal MRI image shows a multicystic ovarian tumor with a diameter of >20 cm and accumulation of massive ascites (A). Contrast-enhanced CT shows a contrast effect on the septum of a giant ovarian tumor (B). The tumor was partially ruptured, leaking and filling the abdominal cavity with jelly-like mucinous contents (C). The ovarian tumor was diagnosed as a mucinous borderline tumor with no noticeable cellular atypia, although some cysts showed protrusion of the epithelium into the lumen and cellular multilayering, and the appearance of island-like free cell masses in some cysts (D). The appendix exhibits massive mucus deposits on the serosal surface, but no neoplastic growths on the mucosal side of the lumen (E).
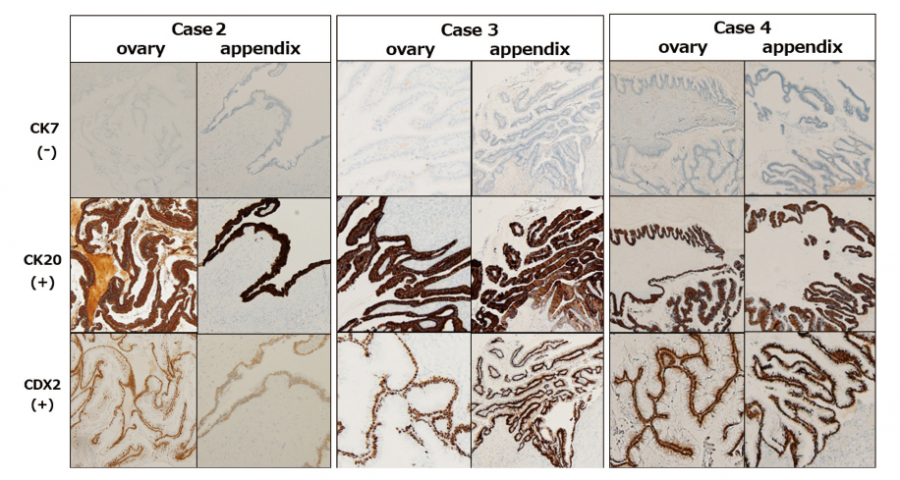
Fig. 3. Immunohistochemical staining findings in cases 2-4.
In cases 2-4, immunohistochemical staining showed that both appendiceal and ovarian tumors were CK7-, CK20+, and CDX2+, findings indicative of a primary appendiceal tumor.
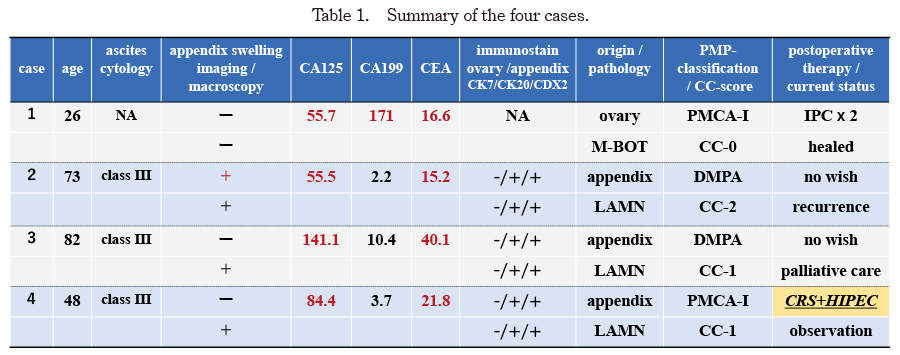
Table 1. Summary of the four cases.
M-BOT:mucinous borderline ovarian tumor. LAMN:low-grade appendiceal mucinous neoplasm
IPC:intraperitoneal chemotherapy
DMPA:low-grade or diffuse peritoneal adenomucinosis.
PMCA-I:intermediate or hybrid between DMPA and high-grade or peritoneal mucinous adenocarcinoma
CC-score:completeness of cytoreduction score
CRS+HIPEC:cytoreductive surgery + hyperthermic intraperitoneal chemotherapy
NA:not available
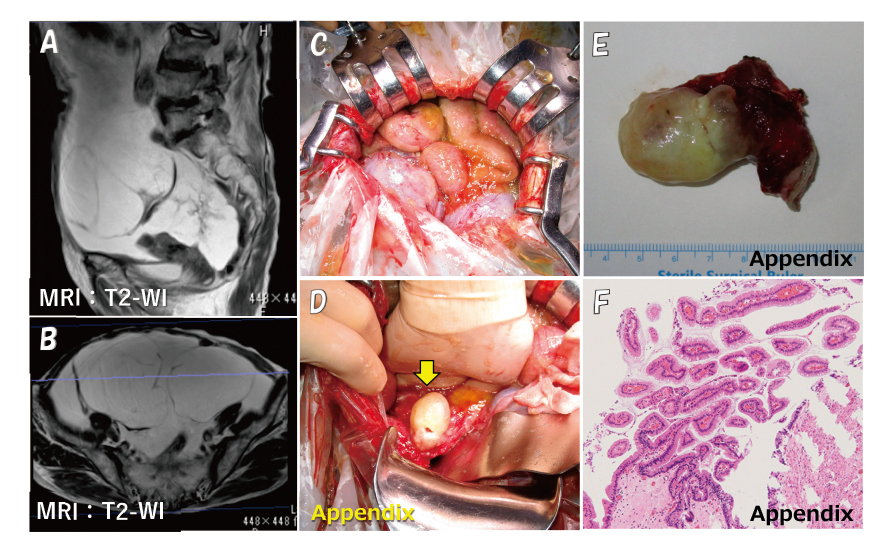
Fig. 4. MRI results, and operative and histopathological findings in Case 3.
T2-weighted sagittal and axial MRI images show bilateral multicystic ovarian tumors with diameters of 9 cm and 14 cm and accumulation of massive ascites (A, B). The tumor was partially ruptured, leaking and filling the abdominal cavity with jelly-like mucinous contents (C). The appendix is mildly enlarged and perforated (D, arrow; and E). The pathological diagnosis of the appendix was LAMN (F).
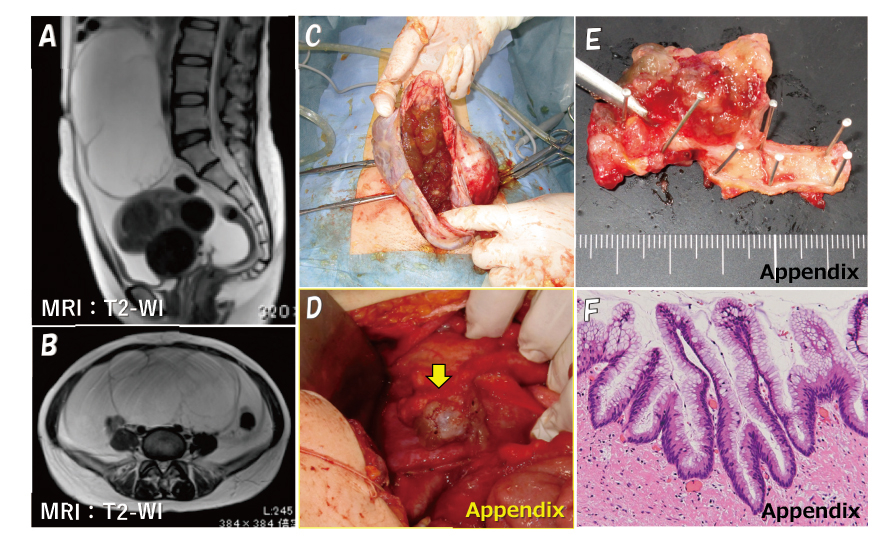
Fig. 5. MRI results, and operative and histopathological findings in Case 4.
T2-weighted sagittal and axial MRI images show a multicystic ovarian tumor with a diameter of 9×14 cm and accumulation of massive ascites (A, B). The tumor was partially ruptured, leaking and filling the abdominal cavity with jelly-like mucinous contents (C). The appendix is mildly enlarged and perforated (D, arrow; and E). The pathological diagnosis of the appendix was LAMN (F).
Discussion
We report four cases of PMP experienced at our hospital. PMP is a disease in which a large amount of jelly-like mucus accumulates in the abdominal cavity (jelly belly) due to perforation of a mucinous tumor, usually in the appendix or ovary. In this condition, tumor cells leak into the abdominal cavity, seed, and grow in the peritoneum. Although distant metastasis is rare, the accumulation of mucinous ascites causes intestinal obstruction or dysfunction, therefore the disease often has a clinically malignant course even if it did not originate from a carcinoma1). Moran et al. reported that PMP is rare, occurring in 1 in 1 million people2). In Japan, a questionnaire survey conducted by the Ministry of Health, Labor and Welfare in 2011 and 2012 estimated its prevalence to be approximately 1.5 per 1 million people1). Gastrointestinal tumors are the primary lesion in more than 90% of PMP cases, with mucinous tumors of the appendix being the most common origin4-6). When the mucus produced by a mucinous tumor accumulates and raises the intra-appendiceal pressure, the appendiceal wall perforates and ruptures relatively easily because of the “blind loop” appendiceal structure. This leads to peritoneal dissemination and metastasis, resulting in PMP5). Many cases of PMP with ovarian tumors are also due to disseminated metastases from appendiceal tumors4,7), and it is estimated that fewer than 10% of PMPs are associated with a primary ovarian tumor1).
Appendiceal tumors are rare, accounting for only about 0.5% of all gastrointestinal tumors8). Tumors are found incidentally in fewer than 1% of tissue specimens removed due to appendicitis9-11). Of these, mucinous tumor of the appendix (MTA) accounts for about 8%12). According to the WHO classification, MTA is classified as low or high grade according to the intensity of cellular atypia, and if the lesion extends beyond the appendix, even low-grade tumors are classified as malignant (invasive mucinous adenocarcinoma, low-grade)13).
Ronnett et al.classified PMPs into three types: low-grade or diffuse peritoneal adenomucinosis (DPAM), high-grade or peritoneal mucinous adenocarcinoma (PMCA), and intermediate or hybrid between DPAM and PMCA (PMCA-I)14). The prognosis of PMP varies widely by grade, with reported 5- and 10-year survival rates of 75% and 68% for DPAM, 50% and 21% for PMCA-I, and 14% and 3% for PMCA, respectively1,14,15).
Contrast-enhanced CT and MRI imaging are useful in confirming the nature of the tumor and ascites, and predicting the presence of distant metastases, peritoneal dissemination, and lymph node enlargement, as well as the staging of the ovarian tumor. In addition, findings of appendiceal mucocele or the findings of liver or spleen serosal surface compression due to myxoma seeding (scalloping sign), although not seen in our cases, may also be useful as a preoperative diagnosis for PMP16-18).
In women with PMP, the coexistence of appendiceal and ovarian mucinous tumors has been found to occur in 1/3 to 2/3 of cases19,20), and Guo et al. reported that they coexisted in 20 (57%) of 35 PMP cases21). Immunohistochemically, CK7, CK20, and CDX2 can be useful markers in the search for primary and metastatic sites when mucinous tumors are present in both the appendix and ovary22). That is to say, the following two types of cases can be distinguished: cases with intestinal origin, CK7-/CK20+/CDX2+, and cases with ovarian origin, CK7+/CK20-/CDX2-23).
In case 1 in this study, the removed appendix was pathologically confirmed to be completely free of neoplastic lesions, and the patient was diagnosed with PMP originating from ovarian mucinous tumor. In cases 2, 3, and 4, on the other hand, immunostaining results led to a diagnosis of PMP originating from appendiceal tumor with ovarian metastasis (Fig. 3, Table 1). In some cases, as in cases 2-4 in this study, the primary appendiceal lesion can have an almost normal shape due to perforation and is therefore difficult to identify on preoperative images. This makes the diagnosis of the primary lesion difficult, and immunohistological studies are therefore important.
As for primary ovarian PMP, there have been reports of PMP due to mucinous tumors arising from mature cystic teratoma (MCT), with Ronnett et al. describing three cases24) and McKenney et al. reporting that 10 of 42 (24%) cases of ovarian mucinous tumors arose from MCT25). It has been speculated that such cases are more common than previously reported, that the original MCT component may be missed when the mucinous tumor is enlarged, and that most primary ovarian PMPs may be of MCT origin24). Ovarian mucinous tumors of MCT origin have morphologic and immunohistologic characteristics similar to those of appendiceal tumors, so their diagnosis requires caution26). PMP of ovarian origin has a better prognosis than that of appendiceal origin, and for PMP derived from ovarian MCT, there are no reported cases of recurrence even with surgical therapy alone27). PMP derived from borderline malignant ovarian tumors also has a good prognosis, so no evidence has been presented regarding the benefit of postoperative chemotherapy6,25,27).
The latest treatment for PMP is multidisciplinary therapy combining complete tumor resection by peritoneal resection with perioperative chemotherapy. In 1995, Sugarbaker et al. reported improved survival with aggressive CRS28), which involves resection of all grossly visible intra-abdominal tumors to the greatest extent possible, and if necessary, with resection of the greater mesentery, spleen, lesser mesentery, gallbladder, right hemicolon, sigmoid colon, rectum, small bowel, uterus, adnexa, upper abdominal peritoneum, and pelvic peritoneum28,29). HIPEC, in which anticancer agents are heated to 41-43°C and administered intraperitoneally for 90 minutes, is generally used for PMP perioperative chemotherapy, because systemic chemotherapy is limited in its effectiveness due to restricted drug delivery to the peritoneal seeding site1,30,31). Recommended drugs include mitomycin C, cisplatin, docetaxel, gemcitabine, and irinotecan, which have relatively large molecular weights, and mitomycin C is most commonly used1,31,32). The size of the residual tumor after CRS is an important prognostic factor for the effectiveness of HIPEC treatment, and Sugarbaker et al. established the CC scoring system to classify this size into four categories (CC 0~3)30). HIPEC is expected to be effective in cases of complete cytoreduction (CC-0 and CC-1; residual tumor size <2.5 mm), but its effect is considerably limited when the residual tumor size is greater than 2.5 mm (CC-2 and CC-3)30,33).
Recently, the effectiveness of laparoscopic HIPEC has also been reported. In addition to being minimally invasive and easy to repeat as needed, the increased intraperitoneal pressure increases the drug delivery into the tumor34,35). In case 2 in the present study, the patient strongly desired minimally invasive surgery and chose a laparoscopic approach to remove the recurrent tumor. If the objective is to remove a single tumor and to perform intraperitoneal lavage, as in this case, minimally invasive laparoscopic surgery should be considered as an option, as it is easier to obtain the patient's consent.
The prognosis of PMP improved dramatically with the introduction of CRS+HIPEC in the 1990s. In 1994, Gough et al. reported that the 5- and 10-year survival rates of patients with PMP (including appendiceal and ovarian primary lesions) were only 53% and 32%, respectively36), but in 2019, Yonemura et al. reported 5- and 10-year survival rates of 76% and 61% respectively (appendiceal origin only)37). Other studies also reported that CRS+HIPEC resulted in good 8-, 10-, and 15-year survival rates of 68%, 63%, and 59%, respectively33,38). On the other hand, CRS+HIPEC is highly invasive and is associated with various adverse events (AEs) and complications that are often severe, including myelosuppression, sepsis, respiratory failure, thrombosis, intestinal perforation, fistula, abscess, and wound dehiscence39). Smeenk and Mohamed reported that treatment-related mortality was 0-11% and the incidence of grade III or higher AEs ranged from 12-68%40,41). As such, adequate informed consent is necessary before administering CRS+HIPEC.
Cases 2-4 in this study involved PMP originating from LAMN, DPAM, or PMCA-I according to the Ronnett classification, and CRS+HIPEC was indicated. The patient in case 3 opted not to undergo any treatment due to her advanced age, and the patient in case 2 wished to avoid highly invasive multidisciplinary treatment. The patient in case 4 was referred to a specialized center for CRS+HIPEC due to a desire for multidisciplinary treatment. Although CRS (yielding CC-1) and HIPEC took more than 11 hours and early postoperative chemotherapy was also performed, fortunately no adverse events occurred for her. The patient is expected to have a good prognosis.
Conclusion
Since female PMP patients are often referred to gynecology clinics for ovarian tumor, even though PMP is a very rare and essentially surgical disease, it is very important for gynecologists to fully understand the pathogenesis of the syndrome. Although the number of facilities that can provide CRS+HIPEC for PMP is limited in Japan42), it is important to consider referring the patient to a specialized facility as soon as possible after diagnosis, in cases where treatment is indicated and desired by the patient.
Conflict of interest
The authors have no conflicts of interest to declare.
Patient consent
We obtained informed consent from the patients for the publication of this work.