Accidental intraoperative hypothermia
Accidental intraoperative hypothermia is commonly observed during general anesthesia because of anesthesia-induced inhibition of normal thermoregulatory control. Core hypothermia during general anesthesia develops in three characteristic phases9-11). Initial core hypothermia results from core-to-peripheral redistribution of body heat when anesthesia inhibits tonic thermoregulatory vasoconstriction. Subsequently, heat loss exceeding metabolic heat production lowers the body’s core temperature in a slow, linear fashion. Finally, a core temperature plateau occurs when the emergence of thermoregulatory vasoconstriction decreases cutaneous heat loss and constrains metabolic heat to the core thermal compartment.
Passive mild hypothermia
The ambient temperature in the operating room is generally low enough to enable mild hypothermia. Therefore, in the early stage of intraoperative mild hypothermia for neurosurgery, mild hypothermia is induced by using the characteristics of accidental intraoperative hypothermia, which is also known as passive hypothermia. Occasionally, the characteristics of thermoregulatory vasoconstriction prevents the body temperature from reaching the target temperature or decreases the cooling rate. It is very important to not only achieve mild hypothermia before the commencement of the main surgery, but also maintain the hypothermic temperature until the procedure is completed. In addition, it is also important to complete rewarming by the end of the surgery so that neurological evaluation can be made (Figure 1). Rewarming is essential for patient management, because sustained hypothermia induces shivering. Shivering is not only remarkably distressing for the patient, it is also associated with a higher risk of an unfavorable outcome, especially in patients with multiple comorbidities and coronary artery disease12). Shivering is also associated with surgical wound infection and an increase in hospital stay12). However, vasoconstriction due to hypothermia can decrease peripheral-to-core heat transfer during rewarming by surface warming, which delays intraoperative rewarming. Therefore, to provide both effective cooling and rewarming, deliberate mild hypothermia is used instead of passive mild hypothermia.
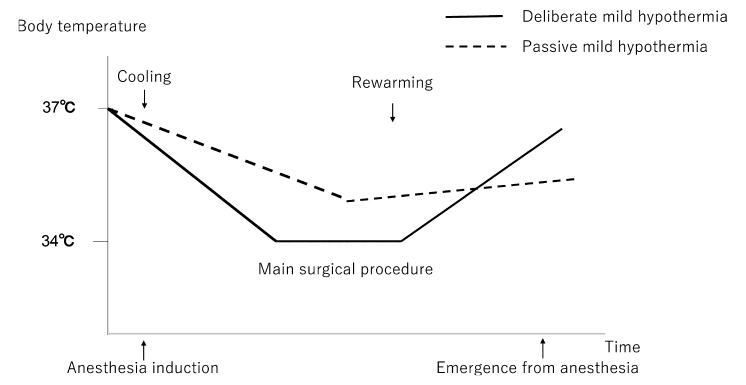
Fig. 1. Deliberate mild hypothermia
The solid line indicates temperature changes during deliberate mild hypothermia. The dashed line indicates temperature changes during passive mild hypothermia. Body temperature after passive mild hypothermia does not reach normothermia at emergence from anesthesia. This situation can cause postoperative shivering at a considerably high rate. There are cases where emergence from anesthesia is intentionally delayed if complete rewarming is not achieved.
Cooling and warming devices
To cool the patient’s body temperature, a water blanket, cooled intravenous fluids, cooling of the ambient temperature, ice packs, and a forced-air device have all been reported to be used.Of these, the water blanket and forced-air device are the most commonly used. In addition, these two devices can also be used for active warming more easily than the other methods, and are similarly effective for temperature management13). However, it has been suggested that the forced-air device may be advantageous over the blanket, because the blanket has a risk of frostbite and thermal injury resulting from prolonged immobilization on a cold or hot water mattress13). Both the water blanket and forced-air deviceare surface temperature control devices; therefore, it has been suggested that the cooling or rewarming rate significantly decreases when vasoconstriction occurs13), and that some kind of countermeasure is required.
Cooling and rewarming methods
Both passive cooling and active cooling have been used for decreasing the patient’s body temperature. Passive cooling is done by setting the room temperature at 18-20°C. At this room temperature, patients’ bodies naturally cool during anesthesia induction8,13). Optionally, cooled intravenous fluids may be used during this period8). Then, the patients are cooled by a water blanket (Figure 2) or a forced-air device (Figure 3), or both (active cooling). These active cooling devices are also often used during anesthesia induction because they can be used to control body temperature independently of environmental temperature (Figure 4). The temperature of the water blanket is set at 5-15°C13-15) and the temperature of the forced air is set at 9-10°C13). A polyurethane-formed pad covered with a cotton sheet may be used to protect the patient from direct contact with the water blanket15). Active cooling needs to be stopped once the core temperature reaches a point that is 0.5°C higher than the target (33-34°C) in order to prevent the after-drop phenomenon. This is a further decrease of body temperature below the target temperature after discontinuation of cooling, and the body temperature is then allowed to decrease to the target temperature. The temperature settings on these devices are then adjusted to maintain the target body temperature. After completion of the main surgical procedure, active rewarming is started with the water blanket set at 41-43°C and the forced-air device at its highest setting13-15). When the water blanket is used for warming, careful attention should be paid to avoid thermal injury. During this period, warming intravenous fluids may be optionally used13). Active rewarming needs to be stopped at a core temperature of 0.5°C lower than normothermia to prevent postoperative rebound hyperthermia16), and the body temperature is then allowed to drift upward. The temperature settings on these devices are then adjusted to maintain normothermia. After the operation, patients are usually awakened and the trachea is extubated in the operating room unless a complication has occurred14-18). However, the patients need to be sedated until their body temperature returns to normothermia.

Fig. 2. Water blanket and heat exchanger
The Blanketrol III hyper-hypothermia system (Gentherm Medical, Cincinnati, USA) is one example of a water blanket and heat exchanger.
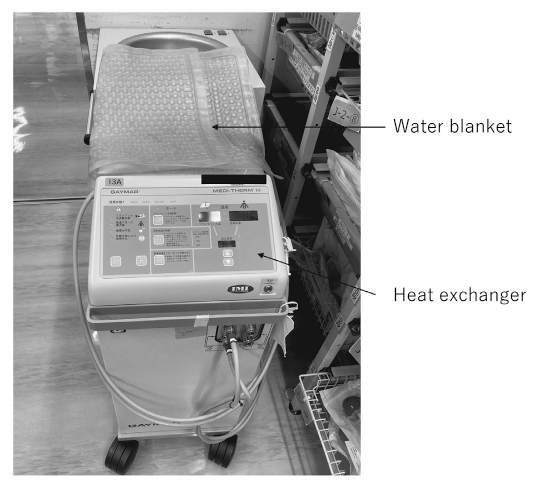
Fig. 3. Forced-air device
Bair Hugger Warming Blanket System (3M Company, St. Paul, USA) is an example of a forced-air device.
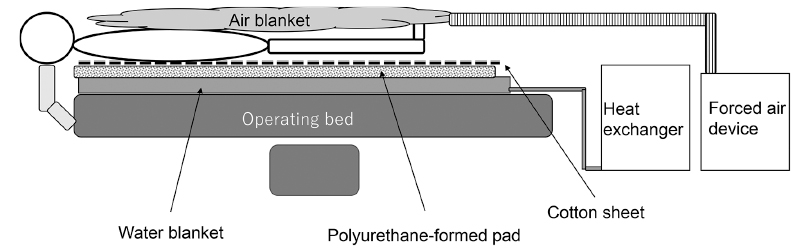
Fig. 4. Intraoperative temperature management
The patient is sandwiched between a water blanket and an air blanket, which are connected to a heat exchanger and a forced-air device, respectively.
Acceleration of cooling rates (Table 1)
Vasodilating drugs may be promising agents to accelerate cooling and rewarming rates during deliberate mild hypothermia because they maintain peripheral circulation and can enhance core-to-peripheral and peripheral-to-core heat transfer when using surface temperature control devices. Several vasodilating agents have been tested during deliberate mild hypothermia. Nicardipine, a calcium blocker, may be used to induce peripheral vasodilation and blood pressure control. In their study investigating deliberate mild hypothermia, Théard et al. reported that nicardipine administered at an infusion rate of 5-15 mg/h failed to counteract hypothermia-induced vasoconstriction13). One patient developed arrythmia and myocardial depression; however, the details and relationship with nicardipine were not mentioned in the article. The authors suspected that the relative hypovolemic status caused by mannitol may have further contributed to enhancing hypothermia-induced vasoconstriction rather than vasodilation by nicardipine13). Prostaglandin E1 (PGE1), which is a potent vasodilator, was tested to examine the effect on the cooling and rewarming rates during deliberate mild hypothermia, and on the incidence of postoperative shivering14). PGE1 at doses of 0.02 and 0.05 μg/kg/min was used, however neither dose affected the cooling and rewarming rates. Conversely, PGE1 at a dose of 0.02 μg/kg/min increased the occurrence of postoperative shivering. PGE1 at a dose of 0.02 μg/kg/min may increase splanchnic circulation more than peripheral circulation19). One possible reason is that this characteristic of PGE1 at a dose of 0.02 μg/kg/min decreased the skin temperature, thereby inducing shivering, because skin temperature is an important contributing factor of postoperative shivering20). From these results, we may conclude that peripheral vasodilating agents are not effective in counteracting hypothermia-induced vasoconstriction during the cooling period.
Dobutamine is known to increase cardiac output and induce vasodilation. Therefore, dobutamine may increase core-to-peripheral heat transfer, resulting in acceleration of the cooling rate. Although it was not a study of deliberate mild hypothermia, dobutamine showed an accelerated decline in core temperature in volunteers anesthetized with isoflurane21), making Dobutamine a promising agent for the acceleration of the cooling rate.
Amrinone is a phosphodiesterase inhibitor that has inotropic and vasodilatory effects. Therefore, like dobutamine, amrinone is expected to accelerate the cooling rate. Amrinone 5 μg/kg/min after a loading dose of 1.0 mg/kg was tested to increase the cooling rate during deliberate mild hypothermia17). Consequently, amrinone successfully accelerated the core temperature cooling rate but failed to accelerate the rewarming rate. It is likely that a combination of the inotropic and vasodilatory effects of amrinone enhances the redistribution of body heat and cutaneous heat loss, and inhibits thermoregulatory vasoconstriction, resulting in an increase in the cooling rate17).
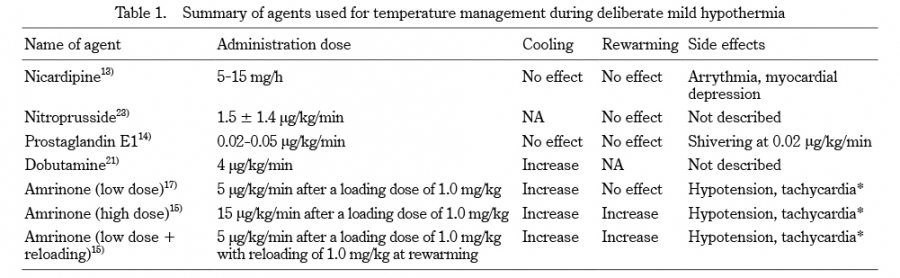
Table 1. Summary of agents used for temperature management during deliberate mild hypothermia
NA; not available, *; Hypotension and tachycardia were observed during amrinone administration; however, they did not affect anesthetic management or require any specific treatment.
Acceleration of rewarming rates (Table 1)
It has been recognized that rewarming is more difficult than cooling in temperature management. Hypothermia may reduce cardiac output as well as increase hypothermia-induced vasoconstriction22). Therefore, hypothermia results in a decrease in peripheral-to-core heat flow coupled with blood flow. Considering that only dobutamine and amrinone accelerated the cooling rate, a combination of vasodilative therapy and inotropic therapy as a minimum may be required to accelerate the rewarming rate.Nitroprusside has been reported to fail to accelerate the rewarming rate, although the details are unknown because the report is only available as an abstract for a scientific meeting23). It was reported that mild hypothermia attenuated nitroglycerin-induced vasodilation24). Therefore, it may be even more difficult to relieve hypothermia-induced vasoconstriction using vasodilating drugs only. As mentioned above, amrinone was previously reported to accelerate the core temperature cooling rate, but not the rewarming rate. In that study, it was suggested that higher doses of amrinone might have increased the rewarming rate17). However, it has also been suggested that higher doses could carry a risk of severe hypotension associated with their use25). Therefore, two methods were tested to obtain a higher amrinone concentrations during the rewarming period in the next trial15). One was a traditional high-dose method (15 μg/kg/min after a loading dose of 1.0 mg/kg), and the other was a new method which, in brief, involved a low dose and reloading at the beginning of rewarming (5 μg/kg/min after a loading dose of 1.0 mg/kg with a reloading dose of 1.0 mg/kg at the beginning of rewarming). These higher doses of amrinone successfully accelerated both cooling and rewarming rates. Patients administered a high dose of amrinone 15 μg/kg/min showed more frequent hypotensive and tachycardia episodes; however, these episodes did not affect anesthetic management or require any treatment15).
Effects of anesthetics on temperature managements
Propofol and volatile anesthetics have been used for anesthetic management during deliberate hypothermia. However, the results of human experimental studies have suggested that a decrease in core temperature caused by redistribution of heat during anesthetic induction depends on the type of anesthetic26,27). This suggests that anesthetics used during deliberate mild hypothermia might affect temperature management. Iwata et al. investigated possible differences between sevoflurane and propofol in the decrease and recovery of core temperature during deliberate mild hypothermia18). A continuous infusion of propofol 3-5 mg/kg/h or sevoflurane 1-2% combined with 50% of nitrous oxide and supplementary fentanyl were used. Finally, it was found that there was no difference in the cooling and rewarming rates between the anesthetics.
Complications induced by mild hypothermia
Deliberate mild hypothermia is relatively safe. Therefore, major adverse events, other than postoperative shivering, are rarely recognized. However, a decrease of even 2-3°C in body temperature can cause adverse events, such as arrythmia, myocardial ischemia, coagulopathy, pharmacokinetic disorder, and wound infection. Hypothermia induces electrocardiographic changes and arrhythmias, especially bradycardia28), which are reversible with rewarming. Frank et al. demonstrated that myocardial ischemia evidenced by electrocardiogram was augmented by 13-36% due to unintentional hypothermia29). Conversely, several human studies have suggested that cardiac ischemic injury may be reduced by mild induced hypothermia28); however, it is reasonable to take extra care when inducing deliberate mild hypothermia in patients who are at risk of cardiac ischemia. Both platelet function and the coagulation cascade may be impaired by mild hypothermia, but fibrinolysis remains normal or is activated; however, these effects reverse with rewarming30-32). It has been reported that hypothermia can decrease drug metabolism. A reduction of just 2°C in core temperature doubles the duration of vecuronium33), and a 3°C reduction decreases pharmacokinetics of propofol by 30%34). These findings suggest that neuromuscular function and anesthesia depth should be monitored. Kurz et al. reported that accidental intraoperative hypothermia increased surgical-wound infection in patients undergoing colorectal surgery35). An increase in postoperative bacteremia was also reported in patients undergoing deliberate mild hypothermia for neurosurgery36). Kurz et al. even suggested that maintaining normothermia intraoperatively was likely to decrease the incidence of infectious complications35). In cases of deliberate mild hypothermia for long periods of time, we should be concerned about the risk of infection. Postoperative shivering is a commonly observed complication of deliberate mild hypothermia. To prevent postoperative shivering, we need to delay emergence from anesthesia until after rewarming has been completed. However, there are several available treatment options for shivering. Meperidine, magnesium or tramadol can be administered to reduce the shivering threshold temperature37,38). Moreover, subanesthetic doses of ketamine can also be used to alleviate shivering39).
Effects of mild hypothermia on outcome
Deliberate mild hypothermia may provide cerebral protection against ischemia during neurosurgery requiring vascular occlusion. However, the effects of mild hypothermia on outcomes were previously unknown. In 1999, a study investigating whether mild hypothermia could be used as a protective therapy during intracranial aneurysm surgery was reported (IHAST I pilot trial)40). This pilot study included 114 patients undergoing cerebral aneurysm clipping with and without acute aneurysmal subarachnoid hemorrhage. Patients in whom mild hypothermia was induced (target temperature, 33.5°C) had a greater frequency of discharge home (75% versus 57%) and a greater incidence of good long-term outcomes (71% versus 57%). However, these values did not reach statistical significance, indicating that a much larger trial enrolling 300-900 patients would be required for that purpose. Six years later, the finding of an additional study, conducted in order to elaborate on the insufficient findings of the IHAST I pilot trial, were reported (IHAST II trial)36). That study enrolled 1,001 patients with subarachnoid hemorrhage who required surgical aneurysm clipping, and mild hypothermia (target temperature, 33°C) or normothermia (target temperature, 36.5°C) was applied. As a result, there were no significant differences between the two temperature management groups regarding duration of intensive care unit (ICU) and overall hospital stay, mortality rate, or the destination at discharge. However, postoperative bacteremia was observed more frequently in patients in whom mild hypothermia was induced. Contrary to expectations from the first trial, the IHAST II trial did not reveal any favorable outcomes. The authors mentioned that the use of colder temperatures for longer periods might have resulted in outcomes different from those of the current study, even though such outcomes were unlikely. Considering that infectious events were higher at 33°C, deliberate mild hypothermia at a temperature that was a little higher might have had different results. Later, Hindman et al. conducted a subgroup analysis of the IHAST II trial41). This secondary analysis was performed using 441 patients with temporary clipping during cerebral aneurysm surgery, who were supposed to receive benefits of mild hypothermia. However, mild hypothermia did not affect the short- or long-term neurologic outcomes of the patients. Until the IHAST II trial, any major adverse events other than postoperative shivering were not recognized as clinical issues; however, The IHAST II trial pointed out that bacteremia could be increased by mild hypothermia. Careful attention regarding the risk of possible infections needs to be paid if deliberately intraoperative mild hypothermia is considered again in the future.

