Case 1
A 74-year-old female with a history of LSS presented to our hospital’s Department of Urology with frequent urination due to bladder prolapse. Physical findings led to a diagnosis of grade 2 uterine prolapse and grade 3 bladder prolapse, based on the Pelvic Organ Prolapse quantification system5). In addition, LSS symptoms of pain in the right buttock and right lower limb were documented by our Department of Orthopedic Surgery.
For more detailed evaluation of pelvic organ prolapse, a pelvic MRI was conducted using a 1.5 T MR scanner (Optima 450w; GE Healthcare, Milwaukee, WI, USA). For cine MRI, an image of the pelvis in the mid-sagittal plane was obtained approximately every 0.42 seconds for 25 seconds using a FIESTA (fast imaging employing steady-state acquisition) cine sequence (repetition time, 4.1 ms; echo time, 1.8 ms; 60 degrees flip angle; slice thickness, 8 mm; field of view, 30 cm; matrix, 200 × 200; and number of signals averaged, 1) while the patient performed Valsalva maneuvers. Other MR sequences, including T2WI and DWI, were the same as those used for ordinary clinical diagnostic purposes.
Cine MRI showed the cauda equina moving in an inchworm-like manner when the patient performed the Valsalva maneuver (Figure 1, Supplemental Movie 1). Uterine and bladder prolapses were also found on T2WI (Figure 2A) and cine MRI (Figure 2B, C). Spine MRI (Figure 3A-D) and CT (Figure 3E-H) performed one year before presentation showed severe lumber canal stenosis at L3/4 and L4/5 due to degenerative spondylolisthesis. Grade 2 lumbar spondylolisthesis in the Meyerding classification6) was found at L4/5, while the lumbar spondylolisthesis at L3/4 was grade 1. In the severity criteria of LSS described by Alsaleh et al.7), severe stenosis (spinal canal area reduced by more than two thirds compared to the normal level at the pedicles above) was found at L4/5, and moderate stenosis (a one-to-two thirds reduction in the spinal canal area) was found at L3/4. T2WI also revealed redundant nerve roots (RNRs). The patient has been followed up, and surgical repair for her pelvic organ prolapses is planned.

Fig. 1. A 74-year-old female with a history of lumbar spinal canal stenosis (Case 1). Cine MRI shows a large movement of the cauda equina in an inchworm-manner during the Valsalva maneuver. The same image is shown in Supplemental Movie 1.
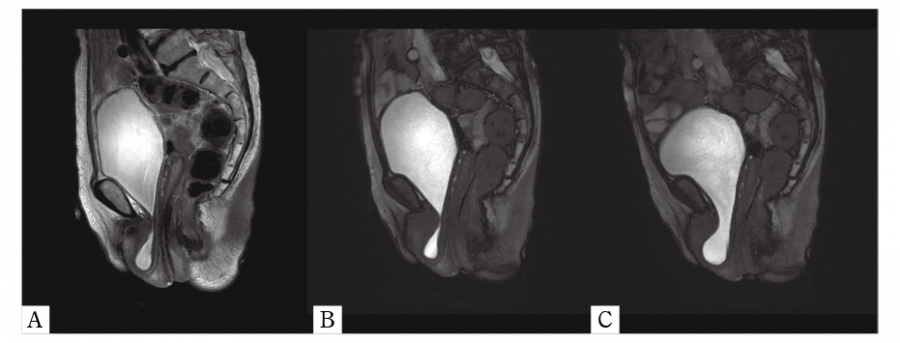
Fig. 2. A. T2WI shows uterine and bladder prolapses (Case 1). B and C. Cine MRI during the Valsalva maneuver also shows uterine and bladder prolapses (Case 1).
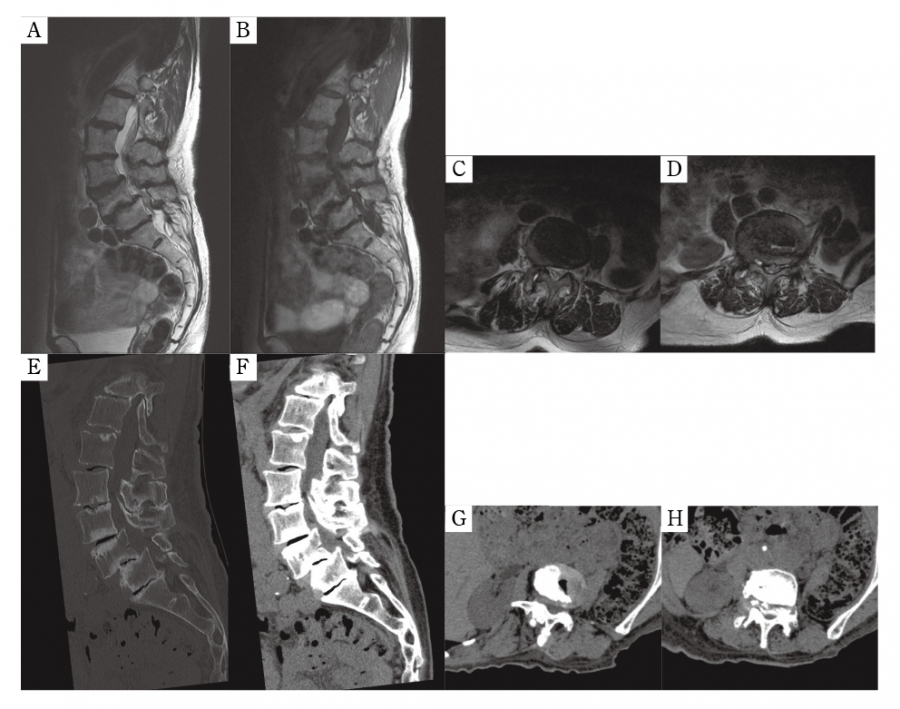
Fig. 3. A, T2WI (sagittal);B, T1WI (sagittal);C, T2WI (L3/4 axial);D, T2WI (L4/5 axial);E, CT (sagittal bone window setting);F, CT (sagittal soft tissue window setting);G, CT (L3/4 soft tissue window setting);and H, CT (L4/5 soft tissue window setting);(Case 1); spine MRI and CT performed one year before presentation showed severe lumbar spinal canal stenosis at L4/5 due to grade 2 lumbar spondylolisthesis in the Meyerding classification, and moderate stenosis at L3/4 due to grade 1 spondylolisthesis.
Case 2
A 73-year-old male with a history of prostate cancer underwent radical prostatectomy and was followed at our hospital. One year after the operation, a follow-up MRI was performed, which included cine MRI for confirmation of urethrorrhea. The cine MRI was conducted according to the same protocol used in Case 1. The cine MRI showed the cauda equina moving in an inchworm manner when the Valsalva maneuver was performed, with movement smaller than observed in Case 1 (Figure 4, Supplemental Movie 2). LSS due to L3/4 degenerative spondylolisthesis was retrospectively found on abdominal CT performed before prostatectomy (Figure 5A-C). Grade 1 lumbar spondylolisthesis in the Meyerding classification and moderate spinal canal stenosis was found at L3/4. The patient is currently being followed and no metastases have been found.
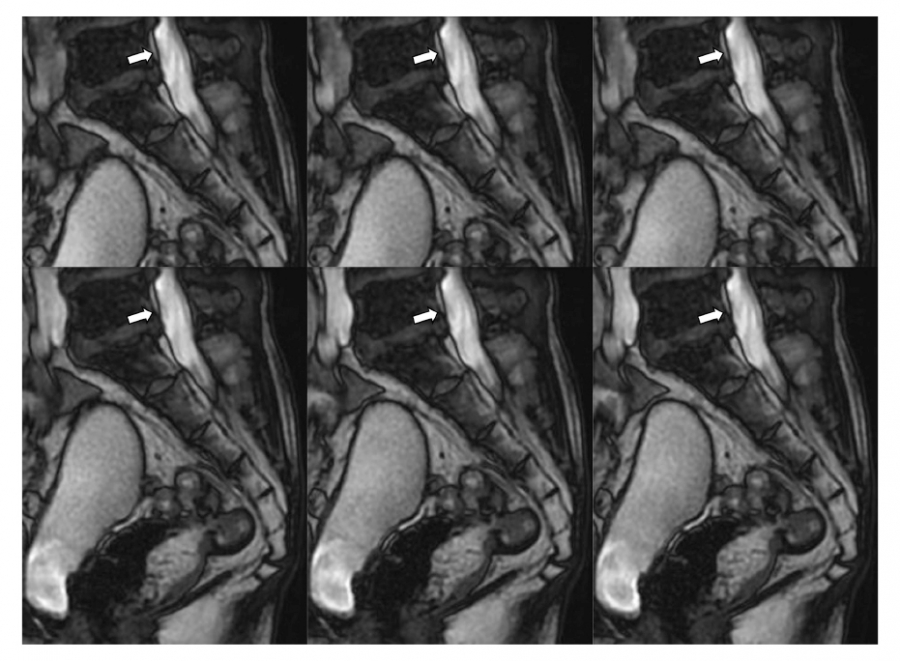
Fig. 4. A 73-year-old male (Case 2). The cine MRI shows a small movement of the cauda equina during the Valsalva maneuver. The same image is shown in Supplemental Movie 2.
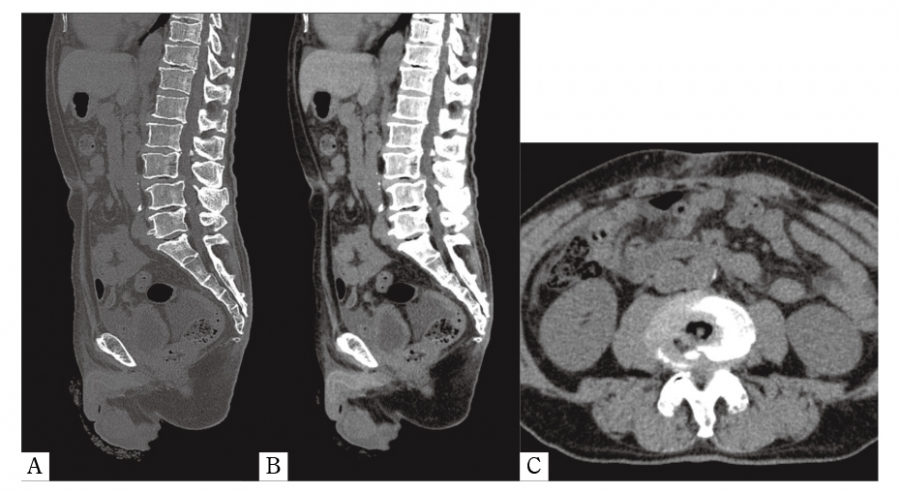
Fig. 5. A, CT (sagittal bone window setting);B, CT (sagittal soft tissue window setting);and C, CT (L3/4 axial soft tissue window setting);(Case 2);Moderate lumbar spinal canal stenosis due to L3/4 grade 1 lumbar spondylolisthesis in the Meyerding classification was retrospectively found on abdominal CT performed before prostatectomy.

